

Don't be ARRsey
Don't get mad about the COVID vaccine ARR (absolute risk reduction) - it's not real

My friend Jessica Rose reminded me of one of her old posts today on the placebo used in the COVID “vaccine” trials and how it might not be a placebo at all. Definitely worth a read here:

The reason we were looking at it was out of a conversation about whether the “placebo” in the Pfizer vaccine trial was saline - as they suggested (and was reported in the infamous NEJM publication, published of course within 10 seconds of submission) - or was in fact saline with “blank” lipid nanoparticles and all the other constituents of the “vaccine” (aka gene therapy vaccine or GTV). At the same time the mice over on twitter were busy responding to this tweet asking whether people thought the study itself was real or not.
Looks like a slam dunk.

But in the replies were repeated references, which I’ve seen before, saying that the ARR was only 0.8%. OK, so? Well, we’ll come to that.
And it got me thinking that there are two issues here:
(1) Why do people on the side of #teamreality repeatedly refer to the ARR (the absolute risk reduction) as an argument against the Pfizer GTV?
(2) What did the Pfizer GTV study (C4591001) actually show?
So I’m going to do a short dig in to show you that the ARR argument is a distraction which you should let go, and explain why.
What is the ARR?
The Absolute Risk Reduction is the actual reduction in risk of something happening in a population. So if you have two groups and 20% of the untreated group get the disease but only 12% of the treated group get the disease the ARR is 8%. In laymans’ terms you could say that you have an 8 in 100 chance of getting a benefit from the treatment. An excellent and fuller explanation is here in a free book chapter.
It’s really the measure that should be used for vaccines and other drug treatments but is very dependent on your prior risk of something. If your risk of the same thing was 2% (e.g. because you’re younger) and it dropped by the same proportion on treatment to 1.2%, the ARR would be 0.8% - similar to that touted as the result in the Pfizer study.
Because the level of reduction or impact of a drug might be consistent across different groups, irrespective of their background risk, and because it sounds more impressive, drug companies will often use the Relative Risk Reduction (RRR) - which is just the % drop in the incidence rate. The same article referred to above gives some examples
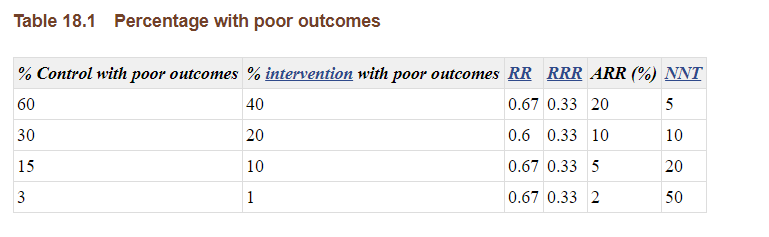
The NNT is the Number Needed to Treat and represents the number of people that you would need to treat to have one beneficial effect - is just 100/ARR. In case you missed it I have given another example last year in regard to the opposite effect - the miscarriages incurred in association with the COVID vaccines:
 and Number ...")
So you can see that the ARR is somewhat more helpful for most people because you can see what the magnitude of the risk reduction is that you should expect from a treatment and how many people you’d need to treat to get a benefit. This is because not only do you need to consider how much the drug works in a particular disease but you have to multiple by the chance of getting the disease (e.g. if the reduction is 50% and the chance of you getting the disease was only 1% before the treatment, the absolute risk reduction is 0.5%).
A corollary might be in cancer treatment where the assumption is that you will die of the cancer without the treatment, and as you are already a cancer patient the incidence of the treated or untreated group would be 1 (or 100%). In that instance the ARR is the same as the RRR.
Of course the pharma companies realise from their experience selling cancer therapies that they will get more mileage out of (more impressive) RRR and so use this in vaccine studies. It’s pretty disingenuous, however in the Pfizer vaccine study the main claim in everybody’s mind is that the drug reduced the risk of infection by 95% (RRR). The corresponding ARR was only 0.84% because the incidence of COVID during the whole (6-week) study period was less than 1%.
I find the paid-off media very helpful in order to dig up claims like this that they believe they have “debunked” as the “fact check” articles usually contain links to the things I’m interested in and that I can’t find easily! In this case:

The numbers are correct. Pfizer correctly claimed their beloved 95% value (RRR) and the Lancet microbe study referenced in the post also correctly claimed 0.84% (ARR). Here is Olliaro’s graphic showing all the numbers together.

However, there is a twist. And the twist is this:
In order to claim that the “actual risk reduction is 0.84%” you have to accept the Pfizer claim of a relative risk reduction of 95%.
Personally I won’t accept discussion of ARR in this study of any percent. You know why? It’s false, because the 95% is false. Here’s why:
What did the Pfizer “95%” study (C4591001) actually show?
So few people know this that it drives me crazy, and I have been going on about it for two years. Hey ho.
They told you. It’s in the NEJM paper and it’s in the VRBPAC submission (see footnote). Note that the NEJM paper was published on the 10th December 2020, which is the same date that the submission to the FDA’s VRBPAC committee was presented. The Pfizer BNT162b2 GTV was “approved” the very next day, with no attempt to assess the 350,000 pages of documentation that the FDA requested 55 years to release to the public.
Here is the full 8 hour podcast of the committee meeting on the 10th Dec (the EUA approval was 11th Dec). Of course you don’t need any time to assess the documentation around a product if you have already decide to approve it!
And the outcome? Just one thing - can you see it?
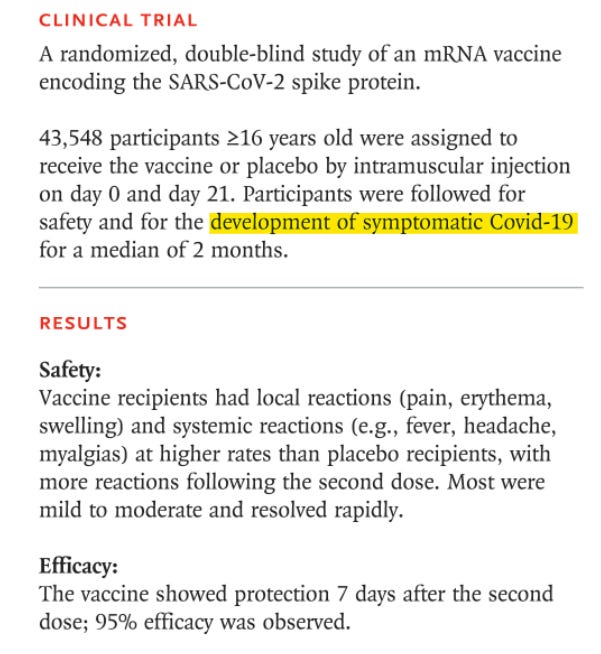
OK the yellow highlighter should help but this is the single finding of benefit in the Pfizer study:
The only clinical benefit recorded in the Pfizer C4591001 study published in the NEJM on the 10th Dec 2020 was: "a 95% reduction in the chance of testing positive for COVID by a PCR test conducted at Pfizer's laboratory in Pearl River"What, you didn’t know? You thought that the Pfizer vaccine had a myriad of magical powers? Nope.
Just to push the point home these are some of the things that people think the Pfizer study showed, but it did not1:
❌ Reduced COVID symptoms by 95%
❌ Reduced COVID symptoms by any amount
❌ Reduced transmission of COVID
❌ Reduced deaths from COVID
❌ Reduced deaths from any cause
❌ Reduced the chance of getting “long COVID”
❌ Reduced the number days taken off work
❌ Reduced COVID hospitalisations or ICU admissions
❌ Reduced the chance of testing positive for COVID by more than 2 months
❌ Reduced the chance of testing positive for COVID at any other laboratory than Pearl River
When you put it like that it’s a bit of an eye-opener isn’t it? Especially: that all the PCR tests conducted in the study were sent to Pearl River (Pfizer’s lab) from all the study site locations in the world. Even if a test were conducted locally, the study authors did not use that test result - only the ones conducted at Pearl River were used for the analysis. Prompting this cryptic tweet to Brook Jackson (who is running the FCA fraud case against Pfizer in the US) in June last year.


This is the document2 that confirmed exactly what went on - taken from the phmpt.org document repository (the one that they tried to suppress the release of for 55 years) just to confirm exactly what we have been saying for 2 years.

And once you had all those lovely Pfizer - analysed PCR tests your study result looks something like this miracle (and nothing like the real world data that we’ve seen that actually showed hugely negative efficacy):

And that perfect graph was behind the fairytale 95% reduction in “PCR-positive symptomatic disease” that sold the product to the world.
Wait, what? What about PCR-not-positive symptomatic disease?
Well. there’s the rub. You know the numbers for this don’t you? Just in case, here they are:
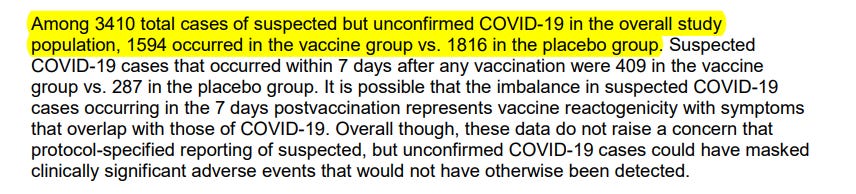
So the effectiveness of the vaccine at preventing “symptoms of COVID” is:
100*(1-(1594/21314)/(1816/21258))… which is 12.45%
Which was the number quoted in another Pfull Pfact™ article that says:

Which means that on the basis of their own data, the probability that the “vaccine” reduces your COVID-like (aka cold) symptoms was 12%, from a background rate of 8.5% (giving an ARR of 0.1%).
Yet they forgot one little teeny tiny important thing - that COVID symptoms include “fever”.
You don’t want fever, it’s annoying and keeps you off work. Because “days off work” wasn’t recorded (if it was, it would have looked bad for Pfizer) we have to use the proxy of fever and include it in our calculation. It’s in the documents in the footnotes and remember fever includes “chills”…
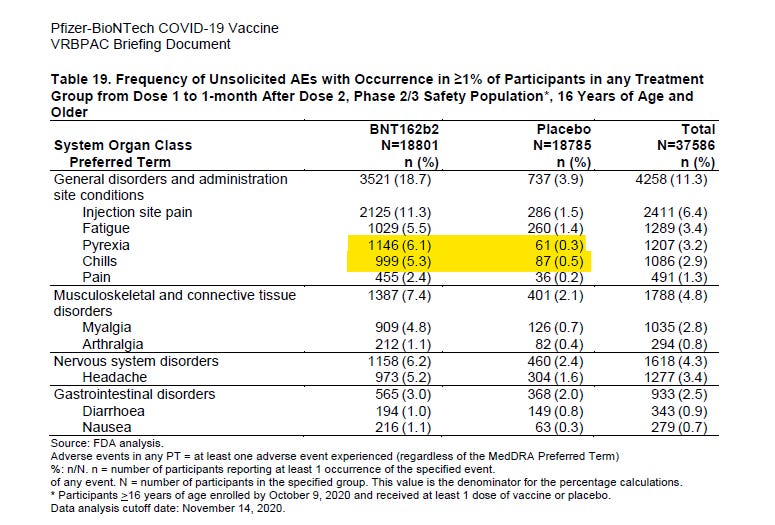
In the BNT162b2 group there were 2145 cases of fever/chills and in the placebo group there were 148
Ignoring the slight difference in the denominator from the overall total there was a 14-fold increase in chills or fever sufficient to report. These should have been included in “COVID symptoms” but they weren’t, because they were dismissed as being a vaccine response
It doesn’t matter. If you get a treatment to prevent a fever and that treatment gives you a fever, there is no net benefit. You might as well forget it. So if the treatment increases the risk of you getting a fever by 14 times, in order to reduce the possibility of snuffles by an eighth, it’s a really shitty treatment. But let’s add in the numbers.
COVID symptoms in “treatment” group = 1594+2154 = 3748
COVID symptoms in “placebo” group = 1816 + 148 = 1964
We can now count our vaccine efficacy against COVID symptoms as:
100*(1-(3748/21314)/(1964/21258))… which is NEGATIVE 90%
Yep. That’s right. The vaccine group had nearly double the incidence of COVID symptoms - from 9.2% to 17.6% which was an absolute risk increase (negative ARR) of 8.4%
Is the first time you’ve heard that? The first time you heard that the Pfizer vaccine study itself showed that the treatment massively increased the risk of you having symptoms that you were meant to be preventing. So you see, arguing about whether the ARR is 0.8% or 0.1% or any percent is a distraction because in their own study showed that any actual reduction in the risk of a respiratory infection could not possibly be real.
To recap:
The ARR (absolute risk reduction) is just a surrogate for the RRR (relative risk reduction). If you agree that there is a beneficial ARR you agree that the vaccine study result was real, when all the evidence in the world is telling you it wasn’t. Don’t be sucked in to this debate.
Well, at least one thing was reassuring in this study - and that brings us back to the placebo. Because the placebo arm had hardly any side effects relating to the injection it is a good bet that the placebo was actually a placebo. Saline. No funny business3.
So, as I’ve said before - focus. Don’t be distracted by stories.
The Pfizer vaccine trial was real, but the results were not.
You were scammed. Don’t let yourself be scammed again.
And, please don’t be ARRsey if you get corrected about your indignation that the ARR is relevant. It’s not.

The Astrazeneca study was a different kettle of fish altogether in respect of placebo, as they used the Meningococcal vaccine as a “placebo” in the phase 1/2 parts of the study. The Menigoccocal vaccine has probably the high adverse event profiles of all the traditional vaccines - so of course they used that as their comparator!
Thank you for all your excellent posts Jikkyleaks. For me, this one is the best!
My background is in Pharmacology (PhD). I’m now retired but I worked in Big Pharma R&D so I know a fair bit about pre-clinical, clinical & regulatory affairs. I’ve been sceptical of the Covid narrative from early in 2020 and follow your posts avidly, because I think you are bang on the money. I am simply horrified by the corruption of science which has been exposed through the Covid debacle (but hope some good may arise from this exposé).
When the vaccine RCT results were announced in Dec ‘20 we could see that the Kaplan Meier plots looked dramatic. If you didn’t know better, they almost look like dose/response curves or close correlations in a regression analysis. But, as you say, when we drill down into the protocols we can see that they are just “bean counts” with time, created by those who decide what the “”beans” are, and control how they are counted.
I note that the vaccine is still approved in the FDA Letters of Authorisation, for the “PREVENTION of Covid 19 disease”, because that was the only endpoint for which the vaccine was supposedly “proved” efficacious by being statistically significantly different between placebo & vax in the original RCTs. Everything else pivots off the original RCTs including more recent trials which use antibodies as surrogate efficacy endpoints.
We knew from early in 2021 that the vaccines didn’t PREVENT Covid 19 disease but the public was confused (& still is confused) by the official narrative that this was due to rare “breakthrough” cases or “variants”. The public still believe the vaccines reduce disease severity even though the RCTs never proved this.
My son is a GP who was vaccinated in Feb/Mar ‘21. He & 5 friends (all vaccinated at slightly different times & places in Scotland over Jun/Jul ‘21) ALL got Covid after a weekend together in July ‘21. At this point I knew the vaccines didn’t work. But this experience also made me think the trial was probably fraudulent. How likely was it that Pfizer could only find 8 Covid cases/~20k vaccinated in their 2 month trial but I knew 6/6 vaccinated Covid cases in one weekend? Since then, almost all vaccinated people I know have had Covid and some of them, more than once.
It is totally dishonest for CDC/Public health to claim that the “vaccines work” because the RCTs on which they achieved Approval defined getting (even 1 mild symptom of PCR +ve) Covid as LACK of efficacy of the test substance (ie “vaccine” or placebo). So the endpoint that was used to say that the vaccine didn’t work is now being used to say the vaccine does work. Hearing credulous celebrities thanking the vaccine for their mild symptoms is super-annoying!
As you say, we all get caught up in trying to navigate this maze of data and flat out propaganda so it’s easy to get distracted by the ARR/RRR debate (though I would say one thing about the (fake) ARR was that it was so low, it didn’t really fit with the “raging pandemic” narrative). The bottom line for me is that the “vaccine” is approved for “PREVENTION of C19 disease” - something it clearly FAILS to do. So the FDA Authorisation Letter is based on a False Claim.
I note that Peter Marks announced recently that future approvals will have to be based on RCTs https://endpts.com/next-gen-covid-vaccines-no-more-quick-variant-updates-and-rcts-may-be-required-cber-leader-writes/ though if such trials are essentially manipulated then we’re on a hiding to nothing.
Please keep up the amazing work - the truth will come out!
Call me a bitter pessimist, but what now? We can scream fraud all day and the morons plugged into the propaganda 24/7 don't care, the MSM liars don't care, the white sorcerers in their Harma castles don't care, most of our 'elected officials' don't care (a few gems do- thank you to those exiled and demonised few) and most of all, judicial systems hardly seem to care (excepting a few interesting wins in the USA).
Thanks Ark, in any case. I know you mean well. I know it's useful to point out how absurd our situation is, how deep the damnation goes. If only the world had ears to hear.