Yes, mRNA vaccines are different. Here's why.

Our famous “viral immunologist” and nudger-in-chief on twitter, Dr Graham Bottley, put out this tweet this week using his apparent business account (which we have covered previously).

It was a pretty straightforward challenge, and - unlike Graham’s tweets - every point made below is referenced with sources.
How are mRNA vaccines different from traditional vaccines? Here’s the list
(1) they contain mRNA, not protein or inactivated virus. RNA is an active molecule that is used to hijack the protein making machinery of your cells and produce foreign protein. There is no off switch built into this process.

(2) they contain LNPs (lipid nanoparticles) which are transfectants and transport those RNAs into the cells of the recipient in order to do this. Lipid transfectants are designed to get DNA into cell nuclei. There is no mechanism to stop this happening with RNA. The definitive test to show whether RNA is entering the nucleus is RNA-ISH, which was not performed by the sponsor or regulator. Instead the regulator approved the product despite being given this confocal image in the investigator brochure showing spike protein (green) in the nucleus (blue).

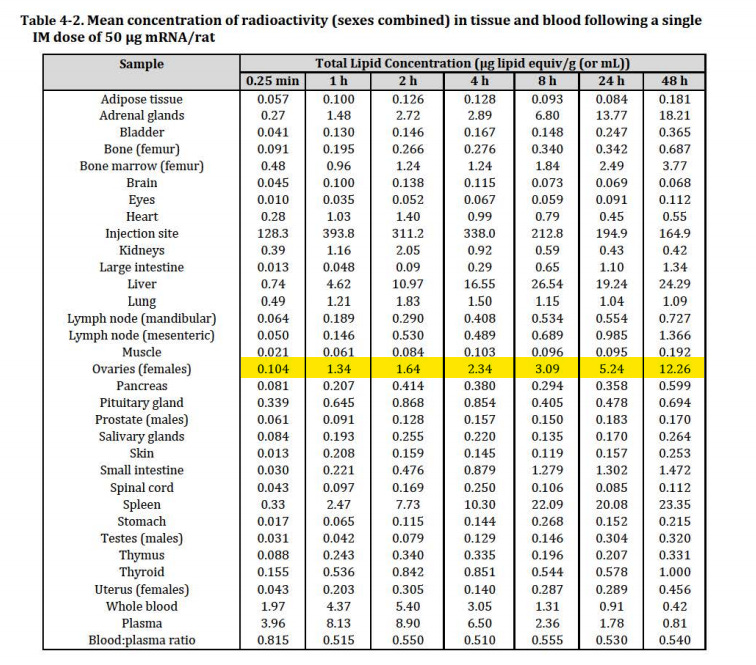
(3) they distribute to and accumulate in the the ovaries and express RNA there, with unknown consequences, and are the only vaccine linked to widespread menstrual disorders.
(4) they are found in lymph nodes still active at least 2 months later with the inevitable risk of T-cell and NK cell exhaustion. In other words, they don’t just act at the time of injection. There is no way to remove them until they eventually degenerate.
https://pubmed.ncbi.nlm.nih.gov/35148837/

(5) the protein they produce for over 2 months interferes with p53 activity leaving the cells they transfect at risk of HRD-driven (homologous recombination deficient) cancers. Discussed at length previously:
(6) The LNPs have their own toxicity profile in addition to the RNA component

(7) The RNA sequences contain oncomirs, microRNAs which have been shown to be carcinogenic. Because they don’t contain RNA, traditional vaccines don’t contain oncomirs.
(8) the proteins produced by the LNP-mRNA have not been sequenced or identified as being the proteins intended, as opposed to recombinant vaccines in which the proteins have to be assessed by the regulators as pure.
(9) COVID mRNA vaccine sequences contain g-quadruplexes that can interact with Glycine zipper fragments and produce prions. No other vaccines do this. These interactions can occur in or around the cell nucleus where the proteins are produced in the vicinity of the mRNA that is still present. Not one regulatory body has assessed this risk.

(10) the 3'UTR of the mRNA (part of the backbone in which the RNA sequence was inserted) was only tested in mice by Ugur Sahin's group in 2019 and never tested in humans prior to a global rollout of the vaccine which used it.

(11) the 3'UTR (essentially a biological adjuvant) contains sequences of human RNA coding for a tumour suppressor (AES) and ribosomal RNA. Traditional vaccines (the ones that work) don’t have human RNA in them. It is completely unknown as to the consequences of using this adjuvant in humans because there was no separate study performed in humans to assess it.

(12) the possibility that the immune system might react against the human RNA (or other constituents, or the cells infected by the RNA) in the vaccine means that there is a risk of severe and intractable autoimmune disease arising as a result of using this RNA. Lupus and other autoimmune diseases have already been reported in relation to COVID-19 vaccination

(13) The risk of myocarditis, thrombosis and death far exceeds all previous vaccines according to VAERS, DAEN and the yellow card scheme
(14) Many other vaccines (apart from those for influenza and dengue) have positive efficacy, which means they prevent disease (i.e. they “work”). The COVID mRNA vaccines have negative efficacy (which means people who get them are more likely to get the infection they are meant to prevent).
The UKHSA were so embarrassed by the negative efficacy of the COVID vaccines they stopped reporting on it in April 2022.

(15) The vaccine study conducted by Pfizer (C4591001) that claimed to reduce infection rate by 95% was so plagued by misconduct that a case is currently underway in the USA to ascertain fraud in this trial. The real world data is so bad that it is not possible that the trial showed genuinely reduced infection rates. Any normal vaccine manufacturer would have been investigated for fraud under these circumstances.
(16) Traditional vaccines don’t kill people from metallic contamination (yes this happened with the mRNA vaccine, and was known about by the regulators - three deaths in Japan, all of whom were young people)
(17) Traditional vaccines have to pass rigorous analysis to ensure the purity of the product. Because the regulators don’t understand mRNA they have no idea whether bumps on an agilent 5200 analysis are additional RNA contaminants or degradation products. The fact that these products were never sequenced suggests that they don’t want to know.


(18) Traditional vaccines only comprise the products shown in the product disclosure statement. mRNA vaccines use your body’s own cells to create proteins but there are multiple reasons why those proteins might not be what was designed. Because of RNA instability, degradation and the use of pseudo-uridine in the mRNA it is not possible to predict the proteins that will be produced (along with the Spike protein intended).
There are likely to be additions to this list but this should do for now.
In the meantime here’s a lovely picture of a sheepdog. This sheepdog is real, as opposed to Graham’s sheepdog. Graham doesn’t have a sheepdog.

This is excellent!! One of the hardest questions for me to answer when attacked by family and friends was how these vaccines are any different from all the other ones we have taken. I used to just answer they are experimental and it’s new technology. This reply always fell on deaf ears.
This is the informed consent information everyone should have had access to before deciding to agree to be experimented on!!
Thank you so much for putting this paper together. I will be sharing with many!!!
Bloody hell, how can that guy be a doctor and still not see the blindingly obvious differences in the technologies. The risks both known and unknown associated with intracellular therapies. The bio-distribution difficulties associated with nonlipids and intramuscular injection. The ability to cross barriers traditionally not at risk of being breached. The uncontrollable dosage being produced which will vary widely from person to person.
Is he really a doctor and immunologist?