BREAKING: Igor just blew the lid off the V-safe pregnancy registry

Amongst the deluge of reveals today1 is a post from Igor that I might have missed if it hadn’t been for the tenacious Josh Guetzkow (🐭) pointing it out. Here is the short substack from Igor that I recommend reading ASAP:

The thing is, Igor is 100% right with this. It comes from a presentation by Lauren Zauche and others made to the CDC on October 19th with an “update of the V-safe pregnancy data” coincidentally after I released this article on October 15th:
Well, if the CDC is reading this blog, they - especially Tom Shimabukuro and Lauren Zauche - are going to need to start thinking about what they have done. The reason?
The safety signal for miscarriage risk related to COVID mRNA vaccines was there for over a year and they knew about it. I’m going to prove it.
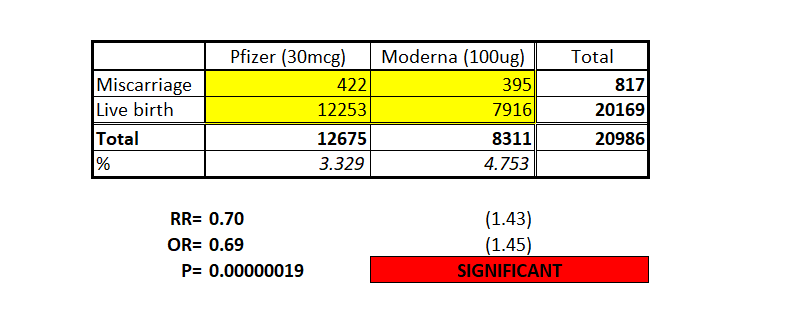
Here is the damning bit of the slide show that Igor refers to:

As I mentioned previously, Lauren Zauche had minimal publications on pubmed.gov before she was recruited for this complex and important research position with the CDC.

Igor is 100% correct that this shows a definitive and significant increase in miscarriage risk for Moderna compared to Pfizer. The risk ratio for this is 1.43 (43% increased) and the p-value is 0.00000019. That is, the probability that this effect happened by chance given these numbers is 1 in 5.4 million. (For comparison that is roughly the probability that the FDA made any viable effort to scientifically assess any of the trial data for any of the vaccines).
In fact the signal for Moderna increasing the risk of miscarriage is so strong that by the time only one-quarter of this cohort of women had been recruited, the p-value (probability that the increased risk was a chance event) was still less than 1-in-a-hundred (p=0.0078). That is the point at which the alarm on the risk of miscarriage should have been sounded, by Lauren Zauche. It was not.
Bear in mind, too, that there is an effective internal control because the Pfizer and Moderna jabs were mostly considered interchangeable. What that means is that there is no obvious confounder that would mean someone would be more likely to have a Moderna jab than a (more recognised) Pfizer jab earlier in pregnancy when most miscarriages happen. In fact it is likely to be the other way around making the difference above an underestimate. So it looks like Viki Male gets this wrong (again) - and gets called out by Jonathan Engler.

However, the data paints a much worse story that was being hidden in this presentation. Those paying attention will note that I criticised Zauche for not understanding the way that miscarriages are counted and for using bizarre methods in her paper published in the NEJM (of course) last year. To recap, her paper suggested that the miscarriage rate in the vaccinated was over 12% and this was “normal” (it is not, as I discussed extensively in “the curious case…”). Her calculations were bizarre because they were performed by rolling week instead of just following a cohort.
Well, we now have the miscarriage data for the cohort (number of miscarriages divided by number of women who were pregnant) ….
….and it shows an overall miscarriage rate of “4%” (841/20726).
Wait, what?
The same cohort that Zauche published in October 2021 where she claimed that the 12%+ miscarriage rate was normal now has a miscarriage rate of 4%? How can this be?
Here’s the explanation and it shows how bad this data is for the miscarriage safety signal. It’s all about the denominators. You see, the denominators in that table are disingenuous. Here is the distribution of doses:

The actual denominator that should have been used is the First trimester (N=6352). In this slide, peri-conception is actually pre-conception as it is before the last menstrual period before pregnancy, so the drug was not given during pregnancy at all. Nearly all miscarriages in pregnancy occur before 14 weeks and are (in this study) defined as a pregnancy loss before 20 weeks. In Zauche’s provisional report, only 11 of 154 (7%) of miscarriages occurred after 14 weeks (14-20 weeks).
So, if we adjust the miscarriage numbers by a factor of 93/100 (to subtract the 7% of miscarriages which occur from 14-20 weeks), then divide by the first trimester figures only, we will get a good approximation to the real miscarriage rate following injection in the first trimester.
I should point out two important things about timing of drug administration in pregnancy at this point
(1) Once past the first trimester the fetus is very robust to most drugs (e.g. thalidomide only had effects in the first trimester; some cancer chemotherapies can be safely given in the second half of pregnancy). So the probability of affecting the pregnancy with a novel therapeutic beyond about 16 weeks is very low. It is therefore disingenuous to include those injected past 16 weeks in the denominator for miscarriage.
(2) miscarriages by definition cannot occur beyond 20 weeks so women who had passed 20 weeks cannot be included in the denominator. Either Zauche knows this and is misrepresenting the data, or is not capable of doing this study.
Because the data is not provided by week our best bet is to look at the bulk of the miscarriages, and assume that the vaccines are distributed the same throughout the pregnancy (Moderna vs Pfizer vs J&J). Using the earlier Zauche data we get this more correctly adjusted table:

Now do you see it?
1. The rate of miscarriage across the board is over 10%, which is double the rate that would be expected for confirmed pregnancies over 6 weeks2.
2. The miscarriage rate for Moderna, which is a higher dose of mRNA, is over 40% higher. At over 14% it is nearly 3x the background rate for miscarriages in confirmed pregnancies. This shows a highly statistically significant dose-response and cannot be dismissed.
3. The rate of induced abortion is also higher for Moderna. This should not be the case and suggests that some miscarriages have been categorised as induced abortion.
I wish I could say that this was the only problem with this cohort. There is one more worrying feature and the way it is presented follows the same pattern.
Remember the CDC dogma is “if you repeat a lie often enough, the public - who hold in such contempt that we will never release the data they funded - will believe anything we tell them”
Here is the first lie:

And here is the pattern repeating itself

I’m not going to labour this point (forgive the pun) but by now you will likely be rolling your eyes knowing what is coming. The CDC are going to gaslight you that the risk of major birth defects is “within historical limits”.
This is what they just published:

This is the chart conveniently labelled “Background rate 3-5%”. This is a lie. The background rate for severe birth defects in developed countries is less than 2% (see here and here3).

But note something else. The rate of major birth defects for mRNA vaccines given in the first trimester was 3.7% with confidence limits up to 4.3% - way over the background rates of major birth defects. This is another indicator that this is a real safety signal and not just “the same as the background rate”. We also don’t know what the severity of these birth defects are but we do know that there are neonatal death safety signals being reported.
The data presented to the CDC this week should have been released to the public a year ago. If they were, we would have done the work that Zauche and Shimabukuro should have done. It’s possible that millions of miscarriages would have been prevented.
For now, they have merely attained the infamy of appearing in the Welcome to Gilead meme series.
For the future, I would hope that a much more in depth investigation of exactly why they withheld and misrepresented this data will take place.
Welcome to Gilead. (Part 4)

ADDENDUM: here is the full slide set from the CDC. Note the repeated association of the same names in most “the vaccine is safe in pregnancy studies” - including Heather Lipkind, Allison Naleway and Nicola Klein all of whom have conflicts of interest involving Pfizer4.
Please remember to visit the telegram channel where short items are posted
The most comprehensive modern day cohort study of miscarriage rates by gestational week for confirmed pregnancies (Naert et al) is discussed in “The curious case…” article but is noted here for ease of reference.
https://www.tandfonline.com/doi/full/10.1080/14767058.2020.1852212
Note that historical and global rates of congenital birth defect tend to be higher and not applicable to the current developed world where early anomaly ultrasound is of high prevalence, as well as non-invasive perinatal testing for chromosomal abnormalities (since c.2010). A background rate of 3-5% has no applicability in the US, Europe or other developed countries with high medical antenatal coverage.
Thank you for commenting and showing the Viki Male "debunking", I did not know she commented on my post!
It is amazing how the CDC says "no differential signal was found" in Slide 37, when the differential signal was in Slide 33. (and note the induced abortion 50% difference! Worth another substack post really, I purposely did NOT address it --want to pick it up?)
I believe that Lauren is "inexperienced" and did not realize the damning nature of Slide 33. Nobody at the CDC realized it either and released the slide set. But we found it
As FL-based attorney Jeff Childers proposed in his recent article:
“We need a federal law removing vaccine injury liability shields.
If we do that, if we reverse the state and federal protections for vaccine makers, our long national nightmare will be over. It would instantly kill every single mandate. One tiny federal law would do it. “
Let’s do it! How can I help?
Let's get Children’s Health Defense & others like them involved and pull our intelligence, passion, and tools together.
https://open.substack.com/pub/coffeeandcovid/p/c-and-c-news-friday-october-21-2022?r=ow9vg&utm_medium=ios&utm_campaign=post