"Miscarriages Needed to Treat": a new metric?

EDIT (07:50 GMT 5/9/22) - the meme posted here in the first version of this article has been removed and replaced with the original picture on which it was based. It came to our attention that the photoshopped (and clearly expressed as such) meme was being used - predominantly by twitter accounts in the very same network referred to below - to bully and threaten other twitter users who had the audacity to post the article. Given that this action reinforces the very claims made in this article by demonstrating exactly how this network functions, the point has been made and I have updated the pictures so that we can concentrate on the primary message.
If you’re old enough (or young enough) you’ll know which movie this image is from and who the character is….

I have chosen the image because it seems that there are people in the public sphere who - to those that don’t actually agree with them - appear to be vying for the title of “Childcatcher of Covid”1.
Now, obviously Chitty Chitty Bang Bang is fiction and so we can put the Childcatcher to bed - except we can’t because as most of you will have realised by now we are literally living in a sequence of movies. And in this particular segment the stars of the show are Dr Viki Male (PhD, not a medical doctor), Dr Teresa Kelly and their associated propaganda “disinformation” agencies such as team halo and the 77th brigade’s infamous twitter coordinator Graham Bottley there to set you straight. And just like Roald Dahl’s Childcatcher2 they seem to be an add-on to the COVID show, focusing their efforts on pregnant women3. They tag team on twitter and make sure that you know that COVID vaccines are perfectly safe and effective in pregnancy. Of course it won’t affect them at all because they have already had their children, so that’s OK.
Here they are on twitter telling us all how COVID vaccines don’t cause miscarriage. Except none of these people has conducted a suitable study to show that, so this is somewhere between speculation and disinformation. And without solid data (see below) to support them, if they are wrong about this they could be risking the largest cohort of iatrogenic fetal loss in history.

In fact, they believe in the “safe and effective” vaccine so much that they spend hours on twitter promoting it and telling us how safe it is. Except when you ask for actual data you get the run around.

So now we have that out of the way we can look at one aspect of the COVID vaccine issue that has not really had as much coverage as it should have since I posted about it in October last year. If you haven’t read this you really should, because it explains a lot of the misinformation that circulates around this subject.
The bottom line of this article is that the V-safe pregnancy registry gives us a clue as to what the increase in miscarriage rate is associated with receipt of the mRNA vaccines. It’s about 5%. That is, the baseline rate is 5% and the miscarriage rate in the v-safe registry is about 10%. You will read misinformation reports regarding 70% and 80% miscarriage rates but these are not true, as you will know from the birth rates showing that - although they are down - the drop is around 10%, not 70% or 80%. You may wish to challenge even my 5% and if you do, please provide the V-safe pregnancy data in a raw format that I can verify.
Unfortunately we don’t have any updates on the V-safe registry because - as of the date of this article - there have been none published since I wrote my article in September. Yes, that’s right, 1 year ago. If that makes you angry it should, and you should address this to Tom Shimabukuro at the CDC who is in charge of that data.
But wait, Teresa (and Viki by association) tell you by implication that you are going to die if you don’t get the pregnavax(TM). So, it’s really important. You don’t want to end up like this poor actress pregnant lady obviously - this is almost an iron lung!

Obviously you must go out and get your vaccine because we all know that the COVID vaccines stop you contracting COVID if you’re pregnant might reduce the risk of unspecified events if you get COVID (although there is no RCT evidence of this anywhere, so you just have to take our word for it OK?).
Remember though that every medical intervention has a risk and so when we prescribe an intervention we need to assess - on the same scale or denominator - the potential benefit (i.e. the reduction in risk of adverse outcomes from a severe disease per 100,000 people given the treatment) against the risk of adverse outcomes from severe disease per 100,000 people who don’t get the treatment. This requires understanding of absolute risk reduction (ARR) which we don’t really hear about because all we hear is “XX superdrug will reduce your risk of YY by ZZ%” and in the fact check sphere this would count as “lacks context”.
So it’s time for some context.
The question is this:
How many miscarriages would need to happen after taking a drug (that is meant to prevent ICU admission), in order to prevent one ICU admission of the mother?
This is a new metric. It’s similar to an old metric called “Number needed to treat” or NNT, which is an established way of assessing how useful a drug is in the real world situation. We have not encountered “Miscarriages needed to treat” before because we have never had a drug that is known to cause miscarriage, prescribed widely in pregnancy to prevent a disease that it does not prevent, before4.
 and Number ...")
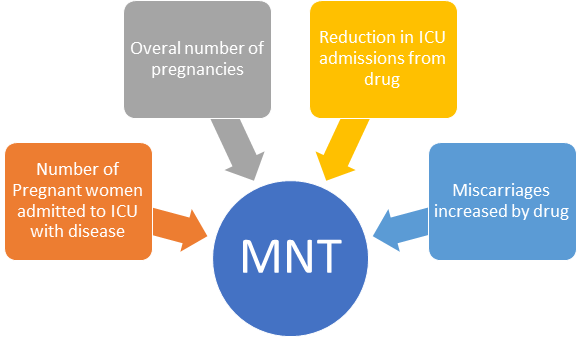
So now we have MNT - miscarriages needed to treat.
In order to calculate this of course we need the following information
(1) What are the overall number of pregnancies in a year
(2) How many pregnant women are hospitalised/admitted to ICU with COVID
(3) What proportion of these are reduced by the “vaccination”
(4) What increase in miscarriages (from a known baseline) occurs in relation to the “vaccination”
We already know (4). We don’t unfortunately know (3) and the way things are going are likely never to know. However the UKHSA reports (which stopped reporting hospitalisation “reductions” from the vaccine after they got a little bit embarrassed) gave some figures in which the reduction could have been interpreted as anything from 0 to about 100% 5. So I’m going for the latest “estimate” from their Week 13 report at about 50%. I being benevolent here, but bear with me.
For the overall number of pregnancies we can get this from the UK national statistics archives. Although this is a year behind real time, this is fine because our COVID data is also historical.
This data gives us for 2021:
624,828 live births
55.8 live births per 1,000 women
[which yields a total denominator of 11.2m age-appropriate women]
This is the number of live births and depending on how you calculate it there will also be a failed pregnancy rate of at least 10% so we can add that to estimate the number of women who were pregnant in 2021, and this gives us (624828/0.9 = 694253 pregnancies).
Now for our MNT calculation we need the probability that a pregnant woman was admitted to intensive care. We can get this from something called the “UK Obstetric surveillance system” that was supposed to be a comprehensive monitoring system for COVID in pregnancy. Funnily enough it has now ended even though “COVID” is more prevalent in 2022 than 2021, but I’m sure there’s a reason.
The data is also published in the ONS statistics here for the time period from December 2020 to August 2021, which is all we have access to. There should be more data available from the UK obstetric surveillance system but that reported in early 2021 and not since. In fact you can tell how disingenuous this group is because they published this in the Lancet (yes, the infamous #Lancetgate journal) in January 2022 which reported on pregnancies up to August 2021 - when only a minority of pregnant women had actually received COVID vaccines.

The closest we can get to the actual data for 2021 is this table, showing in fact how miniscule the proportion of pregnant women who were vaccinated were.

As you can see the age-standardised rate for “double vaccinated” is about a quarter of the “unvaccinated” and that for the single vaccinated is about a third. This data is not verifiable (the raw data is not provided) and given that we have seen from all the UKHSA reports that the early data is only better for a few weeks (in favour of the vaccines) it is surprising that the apparent performance is so poor. We note that much of the performance of these vaccines on retrospective data sets is actually falsely overrepresented due to categorisation bias (as exemplified in Mark Reeder’s excellent piece here which I urge you all to read). So I will stick to 50% as a theoretical reduction for now, being benevolent, however the purpose of this table is really to extrapolate the annualised admissions data.
There were 1895 admissions in 9 months giving us an estimated annualised admissions number of 2527 pregnant women in 2021. Although we can’t get ICU numbers directly from the ONS data (because they refused) the UKOSS paper tells us that (63 of 1148) = 5.5% of their hospital COVID admissions required critical care

This now gives us enough information to calculate the following:
For a pregnant woman in 2021 the following risks applied:
(1) Risk of COVID hospital admission during pregnancy = 0.36%
(2) Absolute risk reduction of COVID admissions6 = 0.18%
(3) Risk of COVID ICU admission during pregnancy = 0.02%
(4) Absolute risk reduction of COVID admission to ICU = 0.01%
So we can now work out the Numbers needed to treat in terms of miscarriages, given the same number of pregnancies in the year = 694,253. Now assuming the 5% additional risk of miscarriage outlined above this would yield 34,712 additional miscarriages for the same year and now we can calculate the following.
The miscarriages needed to treat to prevent one hospitalisation is 5/0.18 (or 34712/(2527*0.5)) = 27.4
The miscarriages needed to treat to prevent one ICU admission is 5/0.01 (or 24712/(139*0.5)) = 500
So there we have it. Given the UKHSA and UKOSS data on COVID, rather than relying on scare stories from twitter doctors who should really know better we now have this:
TO PREVENT ONE ICU ADMISSION FROM COVID IN PREGNANCY WITH THE CURRENT VACCINES WOULD RISK 500 MISCARRIAGES
That’s right - 500 miscarriages.
We can already hear the clamour of objection from the OBGYN institutions, their minions on twitter and their "mutton crew” followers who descend in droves to anybody pushing back against the narrative, so we’ll make this offer:
Open the V-safe pregnancy registry data to public scrutiny without delay and if we are able to show that there is not at least a 5% increase in miscarriage risk I will correct this article with the updated figure, or remove it entirely.
In the meantime we reserve the right to “estimate” - just like the UKHSA have been doing for 2 years. In their own words….

Of course the longer we are kept waiting for this data, the more necessity there will be to make Childcatcher memes, because this question is not going away - however many “nudge units” are deployed to silence us.

For those of you who don’t know (I’m not sure how) the Childcatcher is officially the scariest villain of children’s books.
Ian Fleming wrote the books but Roald Dahl wrote the screenplay where the character was first introduced. https://en.wikipedia.org/wiki/Child_Catcher
I refer to pregnant women throughout this piece in recognition of the empowerment that pregnancy and birth conveys only to women and note that Dr Male (not Dr Kelly) insists on using the term “pregnant people” throughout her monologues.
Well, we did have thalidomide and diethylstibestrol but those don’t matter any more because the children affected were not the children of the people that make the rules, so that’s OK (it’s not).
All reports attempting to provide this figure are plagued with biases. There are literally no randomised controlled trials and only retrospective studies in which the definition of “vaccinated” is highly variable and/or subjective. It is concerning in the least that cohort data from the UKHSA is not provided in this regard and when asked specifically the ONS declined to answer.
Assuming 50% efficacy to prevent hospitalisation/ICU admission as outlined
Wow. I've been reading Igor Chudov so the decrease in births has be obvious in many countries. But this final metric that the covid jabs will cause 500 miscarriages in order to stop one single solitary ICU admission is unbelievable. Wow. Going to post your article elsewhere right away.
Here’s a fact…
If you’re young enough and healthy enough to get pregnant and carry a baby to full term, then your risk group for COVID is a fraction of a percent….