What's your AMH?
Your fertility is not at risk, because the experts said so. Move along now.

You don’t know what your AMH level is? Well obviously you don’t need to know because Kate Clancy, who responded to me disparagingly in May 2021 when I raised this concern, said so:

Now, Kate Clancy is an “expert” in women’s health. In fact she is such a trusted expert that 128,000 women trusted her with their personal menstrual data. Spoiler alert: she removed “woman”, relabeled you “people” or “respondents” and told you that the vaccines didn’t really affect you at all. Thanks, Kate - you’re clearly on our side [not].
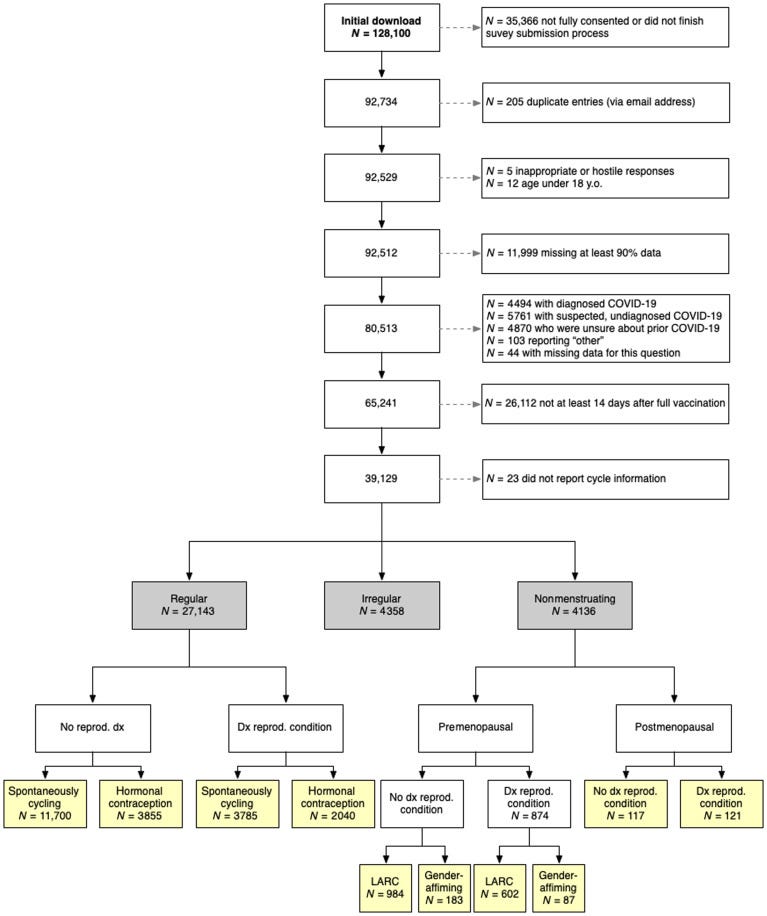
There were 128,000 women recruited to the study but less than 20% were included as can be seen from the CONSORT chart:
You can tell by the article’s use of non-gendered language that this is more of a political article than a truly scientific study. No real biologist would compromise a female-only study in this way, but it’s important for activists like Kate to do this. I mean, you can’t take this language seriously:

Subsequently of course the study concluded that there were no issues that gender-neutral menstruating people should be concerned about.
Just a few problems though….
10% of women (2028/21380) had hot flashes (flushes)*
The number of women who entered premature menopause was not declared.
66% of postmenopausal women had postmenopausal bleeding, which is traditionally a symptom of uterine cancer*
*supplementary data table 5
None of that matters, though, presumably for the same reason that Eric Freed thought it was OK to cover up the potential cancer catastrophe awaiting women described in Welcome to Gilead. This time the author is female, which somehow makes this worse.
Now, it’s possible that all those issues highlighted are benign and temporary. Postmenopausal bleeding could just be a flash in the pan and not actually result in any excess uterine cancers. Note, however, that the first two issues are related - that is 10% of premenopausal women reported hot flashes suggestive of menopause and the number of women entering premature menopause as a result of the injections was not declared.
So how do we work out whether there is a risk of premature menopause - or premature ovarian aging?
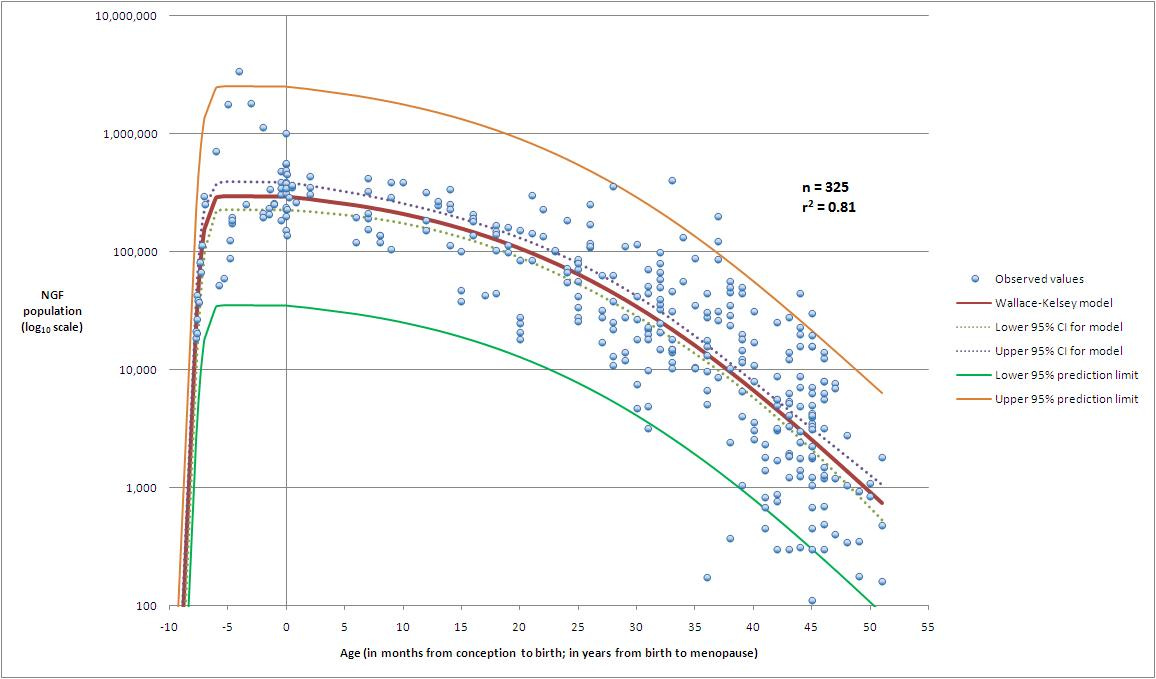
Well, it seems that I’m not the only one worried about this because there are a whole bunch of studies that have been conducted in 2022 relating to the impact of COVID vaccines on "ovarian reserve” - that is the amount of functional ovarian tissue remaining in a woman’s reproductive life. It stays relatively stable until about age 30 when it starts to decline. By the time an average woman is 40 there is insufficient ovarian reserve for most reproductive medicine specialists to recommend the use of own eggs for IVF treatment.
There is, of course, no crystal ball or perfectly accurate way to predict the ovarian reserve as it’s an inexact science. However over the last 10-15 years the field of reproductive medicine has tended to use serum AMH (anti-Mullerian hormone) levels as a surrogate marker to depict ovarian reserve. In general, if your AMH is high you have a good deal of reserve and if it’s low you have little reserve and menopause may occur in the next few years.

So measuring AMH levels was always going to be a battleground for the COVID vaccine fight. Those that were determined to prove that COVID vaccines didn’t cause infertility would be able to show that the AMH levels were not affected by vaccination. And those that were skeptical and had data showing a drop in AMH levels would obviously not be allowed to publish their data.
So what did the “authorised” papers show?
Well, of course they showed that there was no problem. The first and most important paper was that of Mohr-Sasson in Israel (actually most of the papers seem to have come out of Israel, coincidentally) and showed that there was no significant drop in AMH levels.

A scattering of other papers followed the same style and made the same conclusions. It’s worth noting at this point that no other vaccine has required numerous studies of AMH levels before and after administration. It sort of tells you something, doesn’t it?
Anyway, back to the Mohr-Sasson paper that showed no difference in AMH levels in the before and after group. As always, there was just a little problem with the study. The reporting was based on overall numbers (mean and median), but this is not really ideal for this kind of study where you expect the majority of recipients of a drug not to show adverse events. If 10% of your population would be rendered infertile it would not necessarily show up in this kind of study reporting.
What we really need to know is - how many women reported long or absent cycles, or a more than 10% decrease in AMH, and what happened to those women after 6 months?
Well the authors asked exactly this question and found 51/129 (40%) of the study group dropped their AMH by more than 10%. Amenorrhoea rates were not elucidated, which is sadly also a feature of Dr Clancy’s paper

So now we have a study showing that 40% of the population dropped their AMH levels within only 3 months of vaccination, but with no follow-up. Nobody knows what happened to those women. Of course our resident “fertility expert” Victoria Male will reassure you, in one of her commissioned-not-externally-peer-reviewed deliberations, that there is no need to be concerned and please shush1.
However any sensible person, who might be interested in fertility at some point in the future, would be wise to ignore Viki and Kate and simply go and get their own AMH levels checked.
You can do this either before vaccination or after vaccination, or both. Having a record of your pre-vaccination AMH could help you should you require evidence in a court case or class action that your fertility was adversely affected by vaccination (or a vaccine mandate). As with any blood test however, there is a potential for harm (distress) should you find out that your AMH level is not quite as high as it should be. The upside of this is that it might give you an opportunity to act whilst you still have some ovarian reserve.
As you can see from this graph the average AMH level falls over time and also correlates with the “time to menopause”
(note the units, which vary between countries: 1ng/lml = 7pmol/l approx).
 Testing | Infertility Treatments")

So there are really two options:
(1) Listen to Viki Male and Kate Clancy - get vaccinated (with as many #safeandeffective boosters as you can) and hope that your fertility is perfectly intact without any testing.
(2) Get your AMH tested.
It is of course necessary for me to state that Drs Male and Clancy are the declared authorities on this subject, and have been approved by The Wellcome Trust, Twitter and the “Trusted News Initiative”. The approved answer to the above question is therefore (1).
Welcome to Gilead.
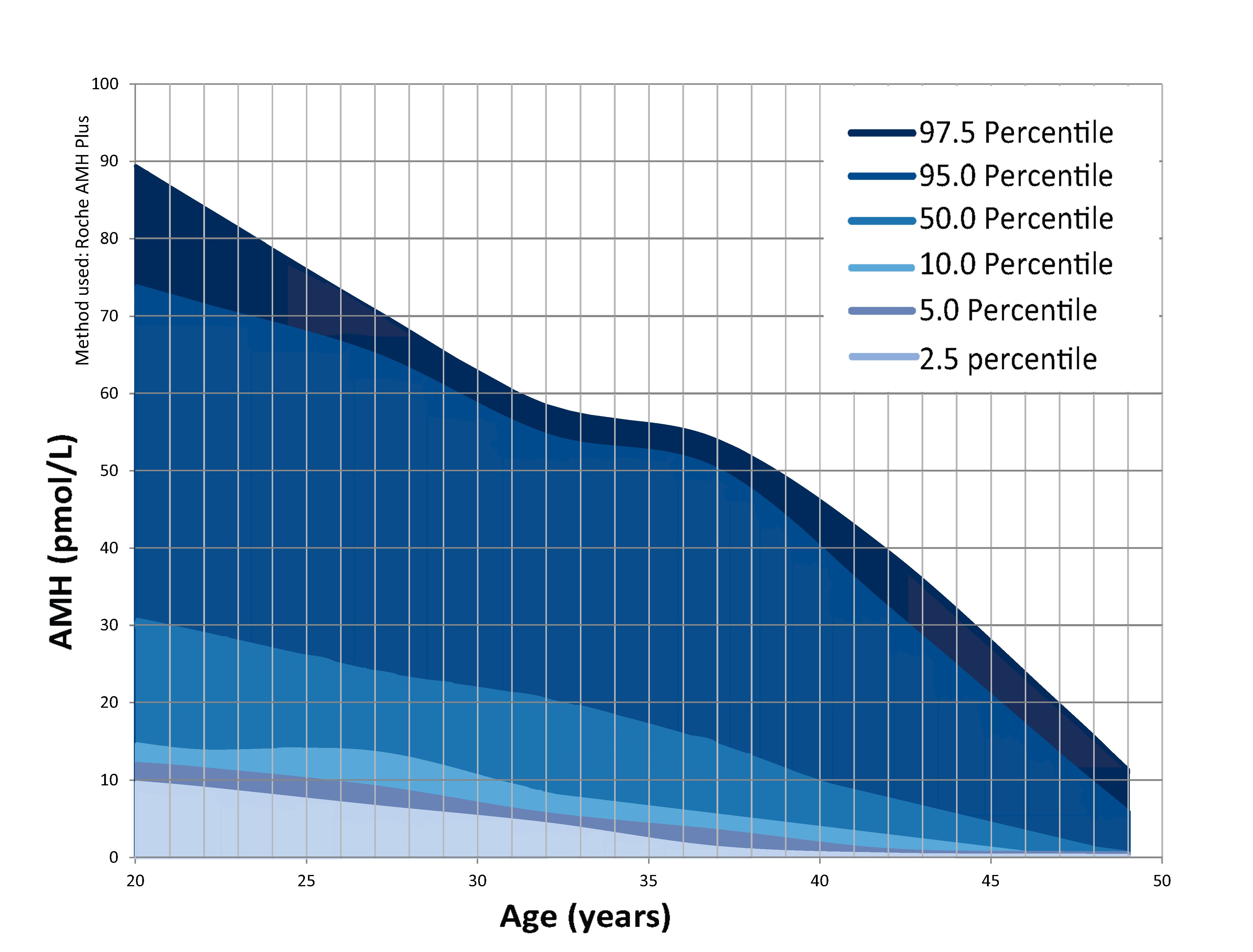
UPDATE: You should find this to be a better graph of the AMH centiles and is based on the Roche AMH assay. The study on which the chart is based is attached below.
Yes, this is now how The Science (TM) works
The gaslighting of women by women experts in this realm is an unbelievable nightmare. If you go read the garbage printed in, e.g., AAAS Science, it's like, "women have had a history of not being heard" and two sentences later, essentially, "people who say these issues [delayed menstruation, 'temporary' infertility, etc.] are problematic and spreading misinformation."
So is it a consequence of profound, systemic medical sexism or is it misinformation?
You can't have it both. You can see why modern 'feminism' is just a window dressing to coerce genuine narratives interested in real human freedom into pro-consumerist agendas.
I find this poll confusing.
<< Do you plan to get your AMH checked (women only)? >>
Can you please define what woman only means?
</sarc>