Would you like some measles with that?
The measles vaccine is the poster child of the vaccine industry... but is it really a vaccine at all?

Well it’s been a few months to get to this article but I think it’s such an important one that it needed the time to make sure I was doing it justice. And it involves one of the central tenets of vaccine science - the measles vaccine.
You see, I’m going to say something that you might not expect, which is that the measles vaccine sort-of “works” - but not in the way you think or you’ve been told.
In fact, it’s almost the polar opposite - and it’s going to shock you.
In order to understand this we need to go back in time to the origin of the measles vaccine.
The Original Measles Vaccine
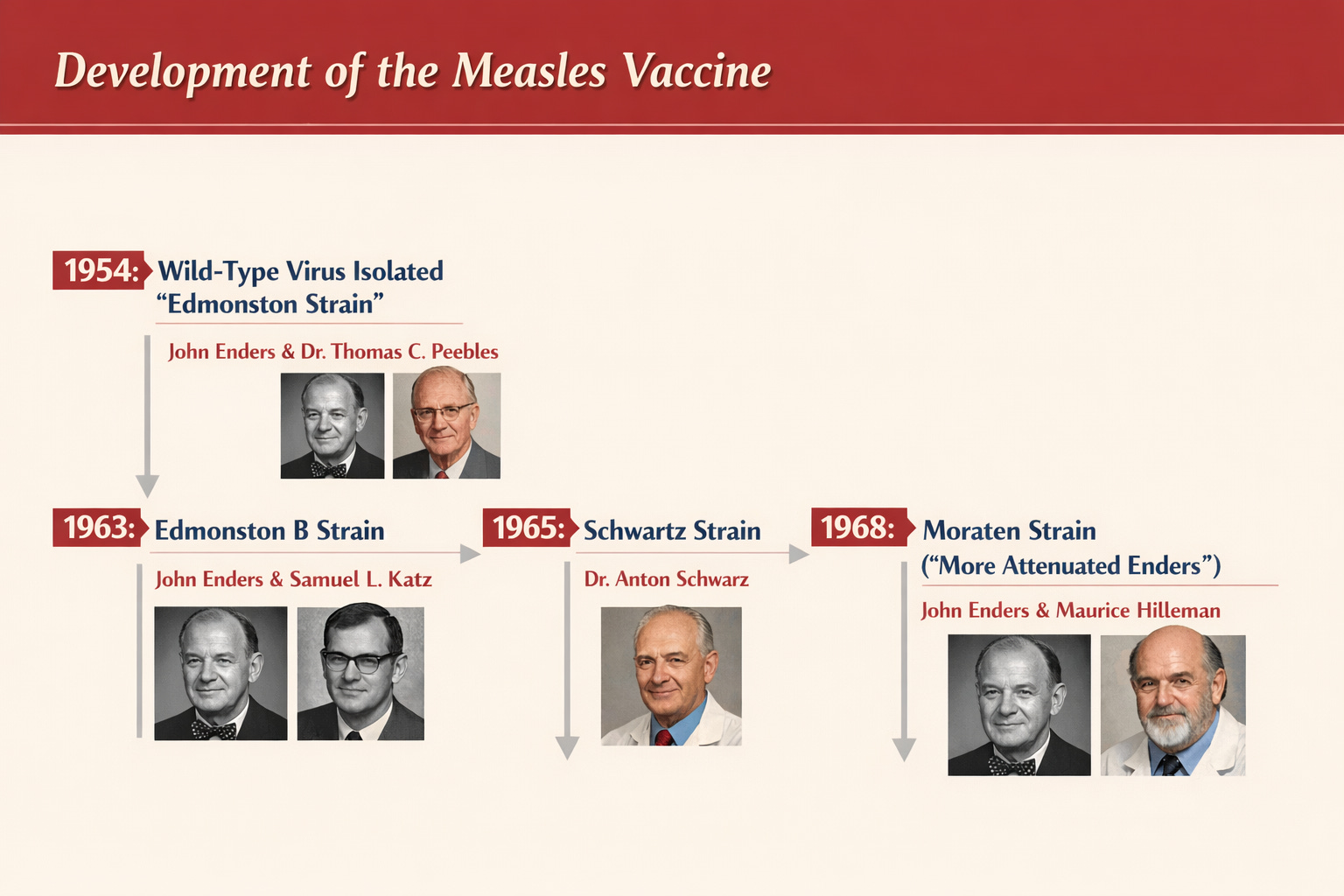
What is commonly considered as the original measles vaccine was developed in the lab of John Enders. What they did was to take a bunch of blood samples from ill students during a measles outbreak in Boston (of course) in 1954. Out of all these samples, despite measles supposedly being one of the “most infectious viruses on earth” they managed to drag out a live version of measles from one of the students - David Edmonston.
Of course, as should happen with 99%+ of measles “victims” (before the Samoa event), absolutely nothing happened to him and he lived a normal life.
So this was the Edmonston “Wild type” strain of measles.
Then, despite this “wild type” measles virus causing no problems to David Edmonston, the Enders lab set about trying to change it to be “less pathogenic”…
…or so the official story goes… and they produced the original “vaccine strain” otherwise known as the “Edmonston B strain”.
The problem is that there is a bit more to it which we’ll come to in a minute, but first an honourable mention to this guy, Professor Francis Home:

Seems like a nice guy. His main claim to fame was as the first Professor of Pharmacy at the university of Edinburgh and later a founder of the Royal Society. But on the path to this celebrity was his work as the first to try to create a measles vaccine - which he did by inoculating children with blood from a person infected with measles.
I’ll just repeat that, given that we now judge historical scientific figures by today’s standards - Francis Home put blood from a measles infected ill person into an open wound of children in order to test his idea. No consent. No care for the consequences.
Here is what Hektoen describes in 1919 in JAMA
So far as known, the first attempt to inoculate man with measles was made by Francis Home in Edinburgh in 1758.… Home ordered a very superficial incision to be made "amongst the thickest of the measles, and the blood which came slowly away was received on some cotton." He then made an incision in each arm of the person to be inoculated, let the wounds "bleed for a quarter of an hour before the cotton was put in, that the fresh blood might not wash off, or too much dilute the morbillious matter."
The cotton remained three days in the wounds.
Home inoculated fifteen children and concluded that in most instances measles developed in mild and modified form.
By the way, this is highly unethical.
The idea that you could believe that a disease was infectious and dangerous and then take blood from an infected individual, make a skin incision in another person and keep a cotton swab in it for 3 days, infested with blood from the infected person (risking skin infection that could have been fatal in the 18th century) is so unethical it’s not funny. But these people didn’t care, because it wasn’t their kids. Just like old Edward Jenner - the “father of vaccines” - who did something similar with someone else’s kid.
So we have the two fathers of vaccinology - Edward Jenner and Francis Home - performing unethical medical experiments on children1.
No problem - it gets worse, though.
Meanwhile it’s worth noting that Jenner was also elected to the Royal Society for his experiments on children, bordering on - if not overt - child abuse.
Which is the basis of all modern vaccinology: the idea that you should infect a child to create immunity to the infection that you’re infecting the child with.
Makes sense, right?
Let’s just pause for a moment there with a little explainer.
In old parlance a vaccine was (per Merriam-Webster 2013):
a preparation of killed microorganisms, living attenuated organisms, or living fully virulent organisms that is administered to produce or artificially increase immunity to a particular disease
Meaning, basically there are two types of vaccines (back in the old days when vaccines were intended to create immunity)
(1) Live organism vaccines (e.g. live viruses)
(2) Killed organism vaccines (e.g. whole or part of dead bacteria or viruses)
We’re not interested in the second one today because we’re talking about measles and pretty much all the measles vaccines in common use are live virus vaccines.
And this is where it gets spicy. I’ll just make the point here:
MOST MEASLES VACCINES IN HISTORICAL AND CURRENT USE ARE COMPOSED OF LIVE MEASLES VIRUS.
That’s not even controversial - it’s openly admitted.
But it’s the next bit that is really the subject of this article - which is this bold claim made by the pharmaceutical companies to sell you the idea of a live measles vaccine:
“THE MEASLES VIRUS IN THE VACCINE IS SAFE,
BUT THE NATURAL MEASLES VIRUS IS NOT”
To reiterate, the Enders lab took David Edmonston’s pretty mild measles strain and did something to it* to make it a “vaccine strain”.
We are mainly going to talk about that strain today because it underpins the whole of vaccinology.
And just to head off the “muh but” campaign from the vaccinologists there were other later versions of the same strains, but they are still all live measles viruses. And as I’ll show there is no definitive evidence that they are fundamentally different from the “wild and mild” Edmonston strain that had already done nothing of significance to David Edmonston.
So what made the vaccine strain a vaccine strain?
I already said that the Enders lab “did something” to the “wild” Edmonston virus in order to make it suddenly safe.
In vaccinology they call it “attenuation”.
How did they do this? Well it’s outlined in the original Enders paper from 19602

For the more wordy of you here is a short extract from the process:
“Seven-day chick embryos were inoculated by the amniotic route … and 6 serial chick-embryo passages were made. Virus of the 6th passage was then propagated in chick-cell cultures. Pooled fluids from these cultures provided the inoculum for the preparation of the primary seed pool. A secondary seed pool was then established and used as the source of virus for manufacture of vaccine B … This was prepared in essentially the same manner as vaccine A. For stabilizing the virus, however, only 1.1 per cent human serum albumin was added …”
All seems lovely right?
Here’s a graphic of the process reminding you that this is done in real life eggs and then chick-embryo cells so vegans should look away now (note that influenza vaccines are still made like this).
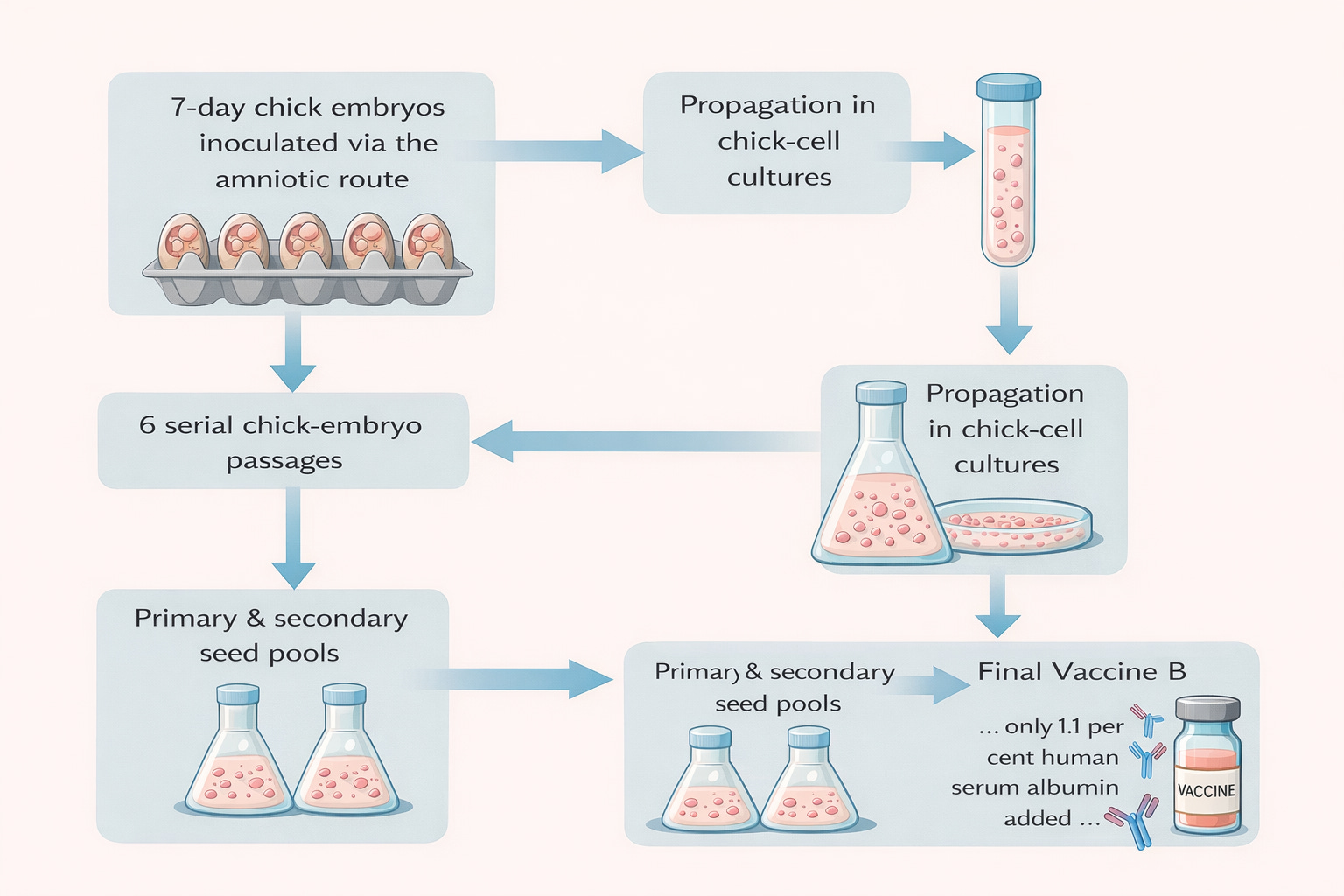
So the process involves injecting a live virus into an egg, letting the developing embryonic cells harbour and replicate that virus (viruses need live cells to replicate). Once they have done that a few times and got the virus to grow they then took the virus stocks and got them to replicate in embryonic cell culture (that is, baby chicken cells) in cell flasks.
And why do they use embyronic (baby chicken) cells?
Because those of you that have experienced a pregnancy will know that embryonic cells grow really fast (OK a pregnancy might seem really slow, but in cell terms it isn’t - it’s as fast as a cancer growth).
This is great for the vaccine manufacturers but might not be so great if those high turnover cell DNA fragments end up in the wrong place. Anyway that’s just a theoretical risk, nothing to worry about I’m sure.

I mean, nobody minds a bit of Avian Leukosis Virus with their vaccine if you’re fighting that really dangerous measles, right?
Anyway don’t take my word for it - this CDC publication outlines the risks of using animal cells for vaccine propagation.

Of course none of that matters to the pharmaceutical industry. And purely because such things are theoretical risks the whole industry moved to “specific-pathogen-free (SPF) chicken flocks”. You know, just in case.
Thank God that our vaccine industry is omnipotent and knows how to mitigate every biological disaster - otherwise we might be seeing a rise in cancer rates or something.
Yeah about that.
“A person born in 1990 has quadruple the risk of colon cancer compared to a person born in 1950”
I wonder what happened between 1950 and 1990?
Coincidentally the Enders vaccine (along with a few others such as the SV40-containing polio vaccines) came onto the market and were rolled out to children across the very Western nations that are seeing this dramatic rise in cancers in people born after 1950.
Of course Business Insider knows that it’s not that - nope, it’s the marathon runners eating processed foods. Obviously.
Anyway, we created a new virus vaccine and we should be able to make a fortune from it by calling it “attenuated”. It should sell like hotcakes.
Perhaps they should have called their new virus/vaccine “Special Chicken Adapted Measles” or SCAM-V for short.

How Attenuated Were the Measles Vaccines?
Let’s just recap a second.
So Enders and friends claimed to have produced a “weak” version of the (non-very-pathogenic) measles virus. And the idea was that they could inject this weak version into kids and they would be protected from measles.
Just like Home tried 200 years earlier, but obviously this time it was going to work..
Sure. But what does “work” look like?
For most people a vaccine that “works” would be something like this:
Child is vaccinated
Child doesn’t get sick from the vaccine
Child never gets infected by (or sick from) the virus
But that isn’t exactly what Enders - and the live vaccine industry (in this case, Merck) were offering.
What essentially they were offering was this:
WE WILL INJECT YOUR CHILD WITH OUR VERSION OF MEASLES,
GIVING THEM MEASLES,
THEN CLAIM THIS PROTECTS THEM FROM MEASLES
Sounds crazy, right?
Obviously the tell tale would be to see exactly what happened to the victims participants of the first measles vaccine trials.
Did they get “measles” - as mild as David Edmonstons’ measles - or did they have no effects?
Fortunately we have the medical journal archives to tell us what did happen.
The Lepow Study (1960)
One of the seminal studies of the new measles vaccine back in 1960 was the Lepow study3, published in the New England Journal of Medicine (one of pharma’s favourite journals).
It was a straightforward study, but unethical.
Why unethical? Well it tells you in the subtitle of the study:
Effects of Vaccine in Institutionalized and Home-Dwelling Children
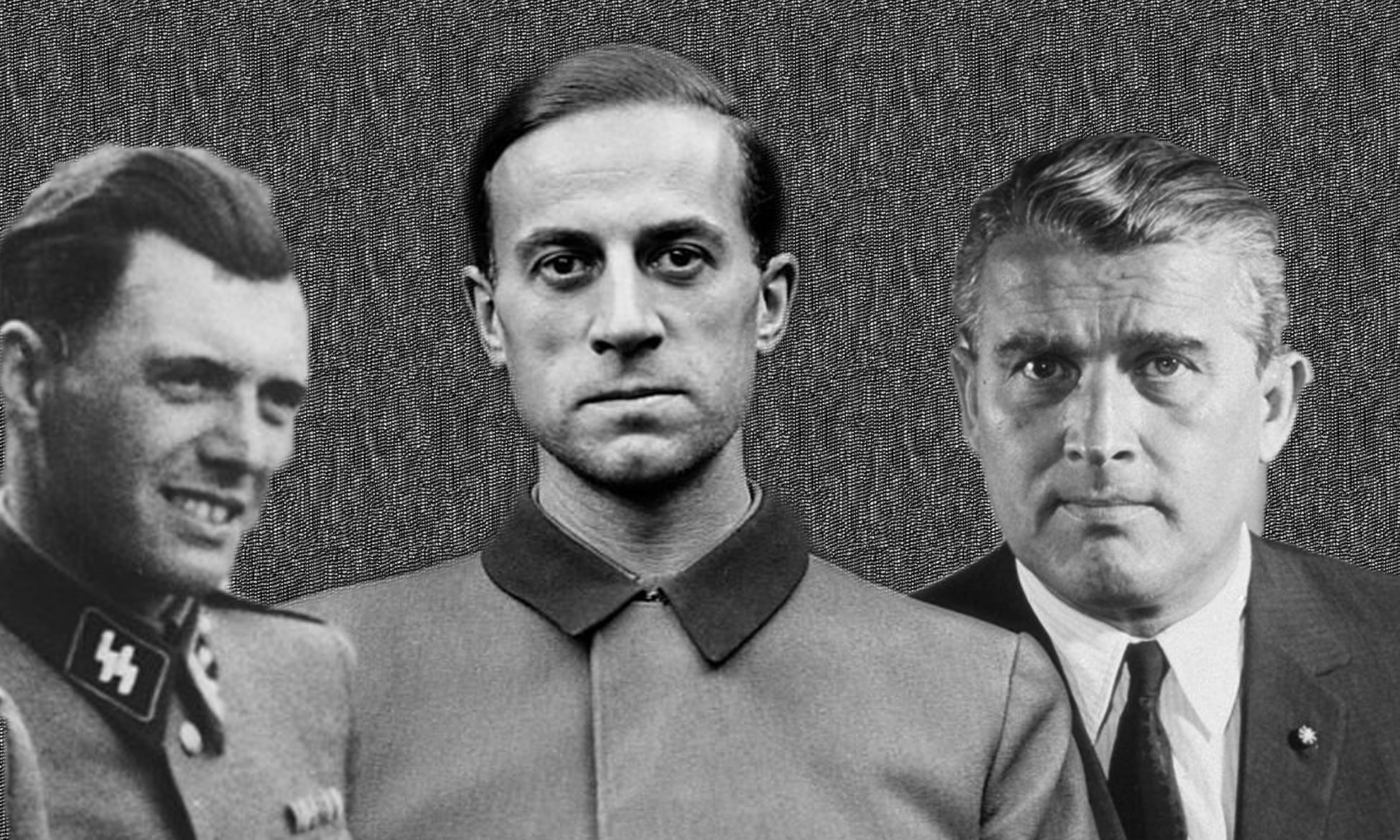
What a lot of people don’t realise is that it’s unethical - under the rules of ICH-GCP and the Nuremberg Code (agreed following the atrocities committed by the national socialists in the second world war where people including children were experimented on by people like Karl Brandt and Joseph Mengele) - to perform medical experiments on children.. because children cannot consent to a medical trial. Granted, their parents can provide consent for them but this caveat was never included in the text of the Nuremberg code - rightly, because the child cannot assess the long term implications of a trial intervention should it go badly wrong.
Here is the actual wording of clause 1 of the Nuremberg code
The voluntary consent of the human subject is absolutely essential. This means that the person involved should have legal capacity to give consent; should be so situated as to be able to exercise free power of choice, without the intervention of any element of force, fraud, deceit, duress, overreaching, or other ulterior form of constraint or coercion; and should have sufficient knowledge and comprehension of the elements of the subject matter involved as to enable him to make an understanding and enlightened decision. This latter element requires that before the acceptance of an affirmative decision by the experimental subject there should be made known to him the nature, duration, and purpose of the experiment; the method and means by which it is to be conducted; all inconveniences and hazards reasonably to be expected; and the effects upon his health or person which may possibly come from his participation in the experiment. The duty and responsibility for ascertaining the quality of the consent rests upon each individual who initiates, directs, or engages in the experiment. It is a personal duty and responsibility which may not be delegated to another with impunity.[12]
It’s really clear isn’t it? Which means that a child cannot consent to be the participant in a clinical trial.
But that didn’t stop Lepow et al who not only recruited children to their trial but instutionalized children.
For those at the back, that means children who were potentially subject to force or coercion by guardians who were not their parents.
Not ethical. At all.
But it gets worse. Not only was this an unethical study but it showed exactly what you would think it would show if you took a child and injected a lives measles virus under the skin…
That is, most of the children got a fever, just like they would get if they were exposed to measles. The reason for this is that they were exposed to measles - just on the end of a needle instead of through the mouth like kids were meant to be exposed to measles. So the researchers gave these kids measles, but it didn’t matter because they were orphans right?
The kids got a bonus too - strep throat, which back in the day could have been lethal. Fortunately penicillin was on hand to counter the effect.
In the orphanage, there was a sharp rise in the incidence of culture-proved streptococcal pharyngitis during the first three days after measles vaccine had been administered. Although none of the susceptible study children contracted the illness, cottage mates were infected. Consequently, all vaccinated children received 250,000 units of penicillin twice daily by mouth for ten days beginning on the third day after they received the vaccine.
All good then. We gave the orphans measles with up to 6 days of fever and strep throat and they didn’t die. Phew. I guess that meant that they got to experiment on them again, just like old Joe from Germany.
Anyway, the kids apparently lived and probably didn’t get measles (again). So I guess the vaccine worked, in the same way that a flamethrower could be considered a fire extinguisher if it burns all the stuff that could catch fire.
But they could have just got measles instead, and not needed the penicillin.
And those pesky “incidental infections” complicated their study significantly, apparently.
One problem that complicated the assessment of he rate and severity of reactions to the vaccine was he presence of intercurrent infections. A fourth of the susceptible children had another illness during he fourteen-day period after vaccination. It is quite possible that some of the respiratory symptoms attributed to the vaccine resulted from infection with other agents.
Anyway maybe that was a one off. Let’s try another study.
The Krugman Study (1962)
This one is a doozy. It was conducted on “Insitutionalized children at the Willowbrook State School” which was a special school for “mentally defective persons”.
So the kids were “mentally defective” and therefore they could consent to a clinical trial… riiiight.
I mean, obviously it’s unrelated because Joseph Mengele’s experiments on “mentally defective” children were clearly different, but it is worth pausing for a moment at just one of the testimonies of the time (and why the Nuremberg code came to be)…
Most of the victims of Mengele’s medical experiments were children. The children Mengele selected for experiments lived in separate barracks from the other prisoners and received somewhat better food and treatment. Mengele was friendly toward the children. In 1985, Moshe Ofer, a survivor of Mengele’s experiments, described his and his brother Tibi’s encounters with Mengele:
[Mengele] visited us as a good uncle, bringing us chocolate. Before applying the scalpel or a syringe, he would say: ‘Don’t be afraid, nothing is going to happen to you…’ ...he injected chemical substances, performed surgery on Tibi’s spine. After the experiments he would bring us gifts...In the course of later experiments, he had pins inserted into our heads. The puncture scars are still visible. One day he took Tibi away. My brother was gone for several days. When he was brought back, his head was all dressed in bandages. He died in my arms.
Anyway, I’m sure injecting live measles virus that had been passaged multiple times through chick embryo cells in a 1950s lab culture didn’t count anywhere near the kind of unethical experiments that Mengele & Co did - especially as the children that were going to receive this concoction were “mentally defective”. Because it was done in the West, and we’re the good guys remember?
Getting back to the point of these (series of) unethical studies conducted for the greater good of “preventing measles by injecting measles”…
What did Krugman et al actually report? Well, this is one of the very few studies that tracked what happened to children who got measles naturally against measles via injection.
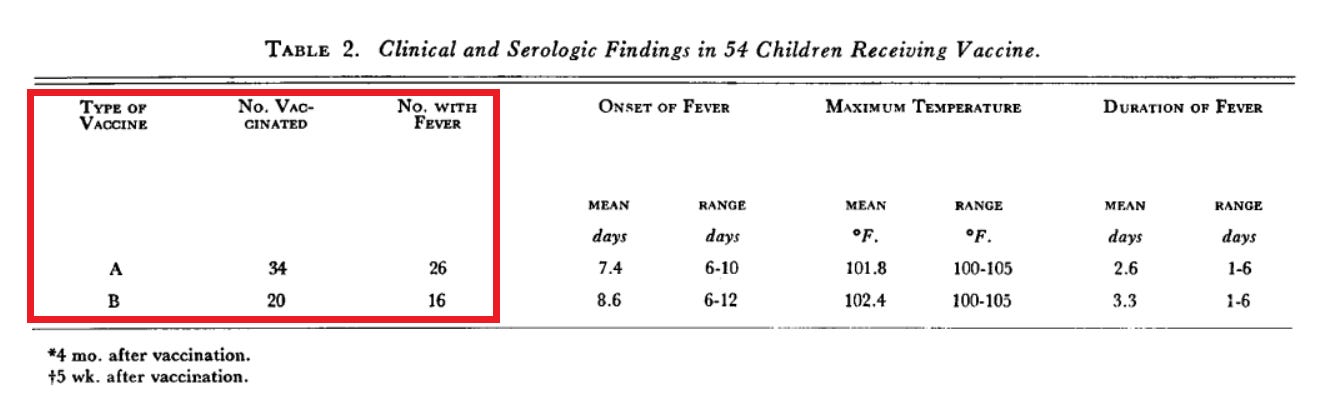
And, unsurprisingly, the rates of fever in both groups were the same:
Of course the people running the study are not going to be inclined to report exactly the same level of fever but it doesn’t make a great deal of difference whether you have a fever of 101 of a fever of 100.9. You still feel terrible.
But wait, “measles isn’t just a fever” I hear you say. And you’d be right, it’s a rash too. And of the children in this study given “vaccine” only - 56% of them developed a rash with an average duration of 2.6 days. And 94% got a fever.
So, they got measles. It’s just that their measles was injected instead of ingested, but it’s still measles.
In fact, these measles (injected vs natural) are so similar here are the antibody titres (blood antibody levels) that the participants of the study showed up to 12 months after the event.
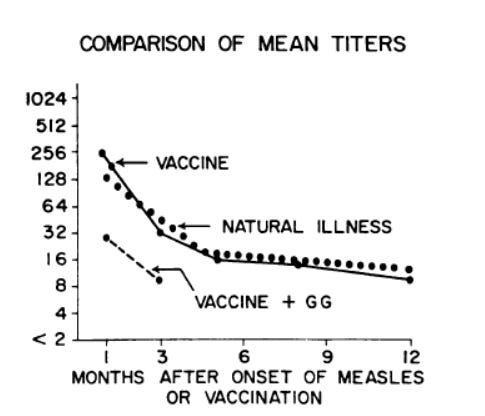
Other studies from the 1960s
Presumably to avoid the risk of harming American children (and receiving bad press) Morley ran a study4 in Nigeria (of all places) with the live Enders vaccine. In stage 1 of this study, similar to the other studies, there was a bunch of “side effects” aka “measles symptoms” after receipt of the Enders vaccine (aka measles).
In other words, the kids got measles. Again. What a surprise.

In fact in this series 100% of the kids got a fever, and that wasn’t all they got. 10/19 (53%) got a rash and 11/19 (58%) got diarrhoea as well as the fever.
Of course the people making the vaccine dismiss the fever as a nothingburger, but so is measles in over 99% of kids.
So what exactly is the injected measles preventing?
We’ll come to that soon. But here’s another study explaining exactly what happened when the injected measles (with chicken cell contaminants) was given to children. This is the Kempe study in 19605 which, again unethically, was conducted on children in care.
These children were studied in the State Home and Training School, Wheatridge, Colorado… In the State Home about 800 mentally retarded children and children severely handicapped by congenital anomalies are cared for and given appropriate vocational training
Presumably the “vocational training” involves being inducted into clinical trials of viruses injected into them that were so dangerous they needed to find a vaccine against them. And if experimenting on “mentally retarded” children is not enough just add some rectal probes. Yep. Gotta get those temperature recordings right.
Beginning on the seventh day after vaccination, a pediatric nurse experienced in communicable diseases visited the inoculated children and recorded the temperature (by rectum) each afternoon, as well as any signs of illness. These observations were continued until the twenty-first postinoculation day
Anyway I digress. This is what happened when the children got their live measles injections (called vaccines).
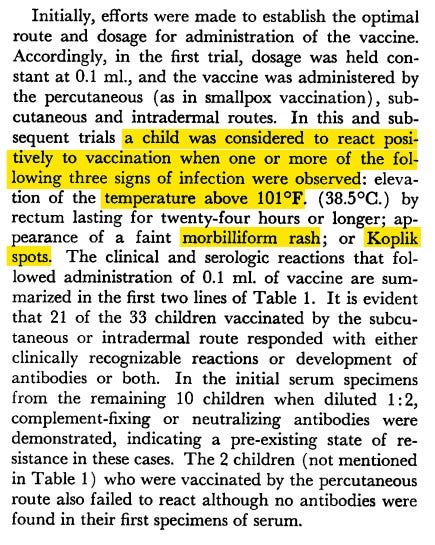
Yep. That “morbiliform rash” and “Koplik spots” is… measles.
Congratulations Dr Kempe, you injected measles virus into “mentally retarded children” and watched them develop measles. With a probe up the bum.
Wow. How could we have managed to develop lifesaving medicines without you?
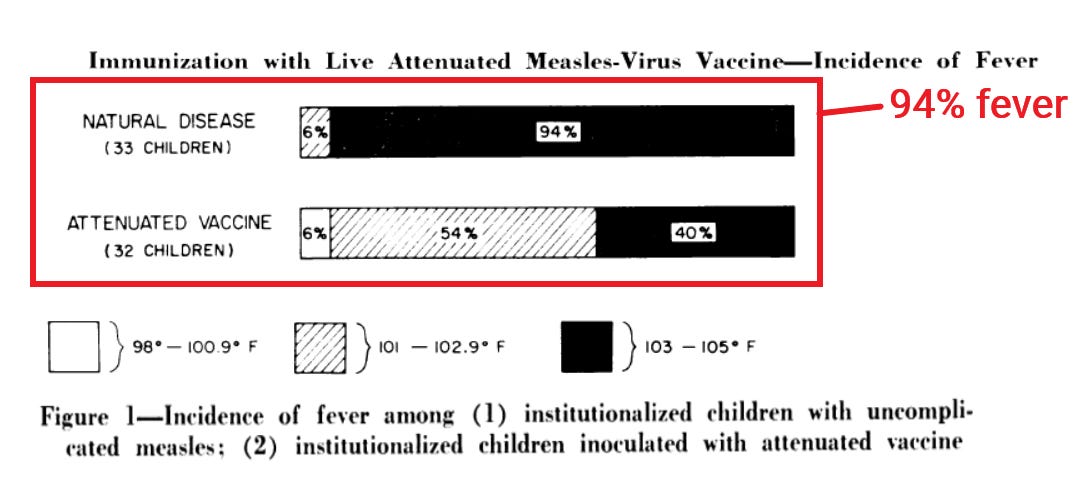
“But”, you cry, “the Kempe study claimed that the vaccine-virus-measles was much less of a disease than real-virus-measles”. That’s true. They did claim that. And it was totally made up. Here’s figure 1.
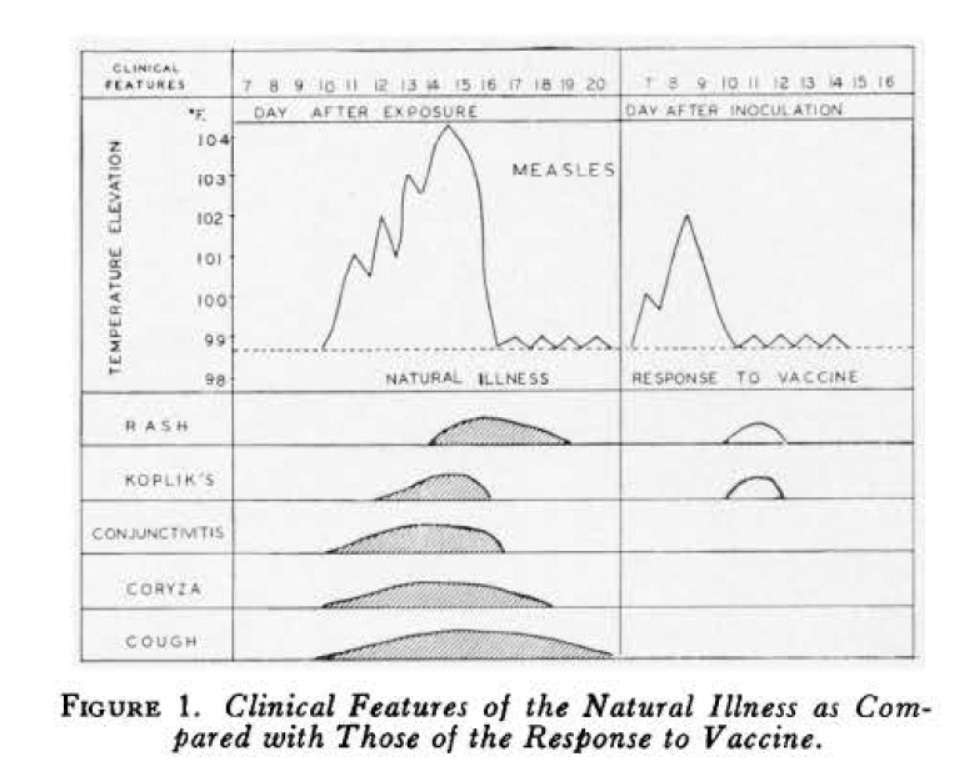
“Clinical features of the natural illness as compared to those of the response to the vaccine”. What a difference.
Yet the left hand part of the chart was totally fabricated as there were no patients with measles in the study at all. You can see the amateurish drawing in the chart once you know that it was made up. They just drew it.
The chart above is so Mickey Mouse it’s actually embarrassing. It’s not scientific in any way.
So, was there actually a clinically valid research study (even excusing the unethical experimentation on vulnerable children) that showed that injecting the “vaccine” measles strain was any better than injecting the “live” measles strain?
Of course not.
But let’s get back to how bad natural measles (not the SCAM-V type) actually is, for which we desperately need a vaccine.
“The most infectious disease on earth”
You will no doubt have heard this line multiple times and it is the primary driver in the push to administer “measles-to-prevent-measles” (aka live measles vaccines) to children.
We’re going to see if it’s even true.
As a typical example here is a recent fearmongering article from The Conversation (one of the media organisations that helped cover up the lab origin of COVID).

It sounds bad, right? Such a scary disease.
It’s written, though, by David Higgins who proudly declares in his papers that he has no conflicts on interest, but forgets to declare his board membership of Immunize Colorado - a vaccine advocacy group which definitely does get its funding from pharma as does his other affiliation - the American Academy of Pediatrics, which gets millions of dollars from pharma….

… and the Childrens hospital at Colorado which also does - a huge amount in fact.
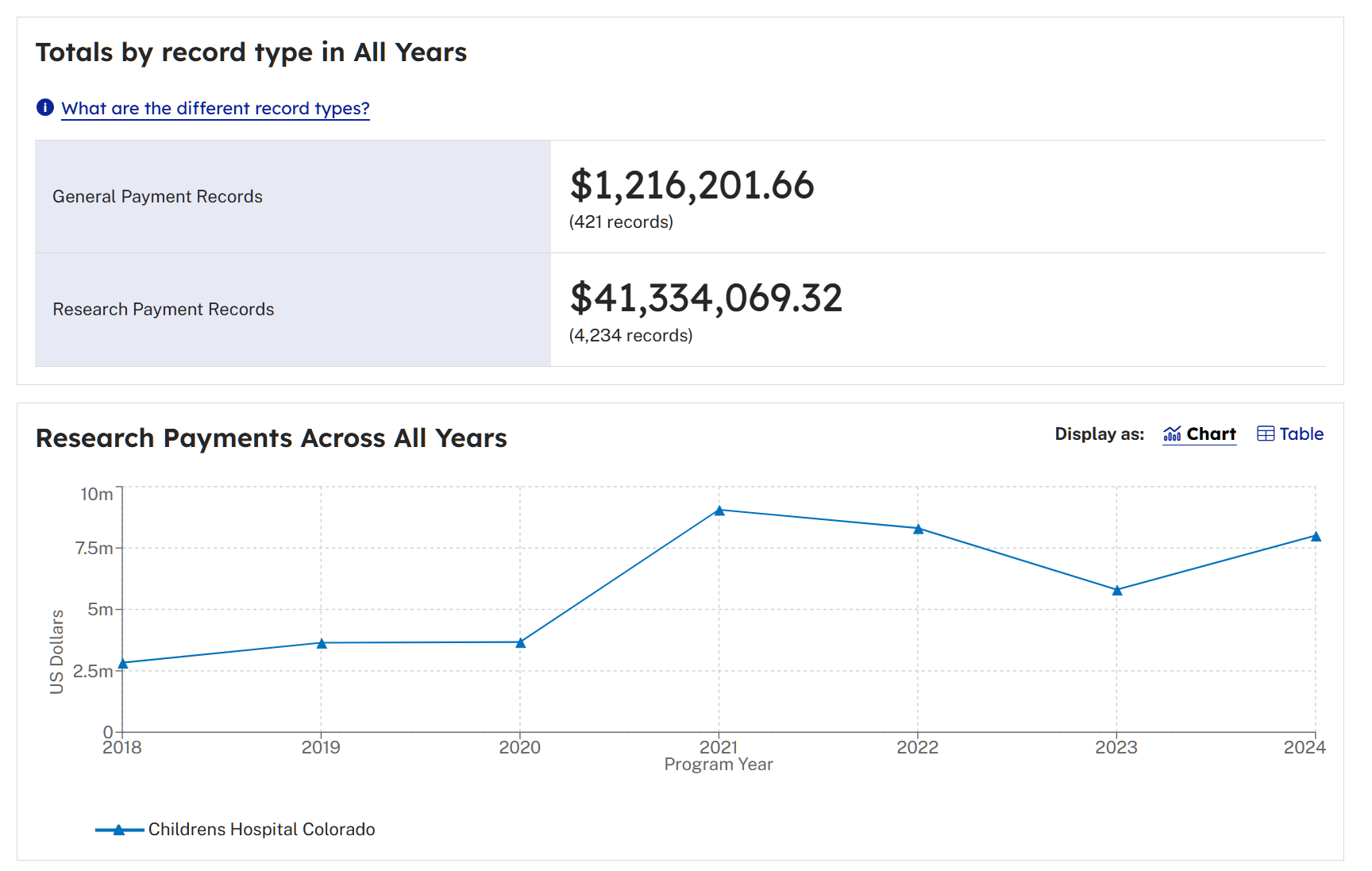
Just to be clear, this is not a dig at Dr Higgins. It’s just that his article is heavily promoted in an internet search and is a very typical example of the kind of propaganda that is written by (or often for) doctors who pretend that they have no conflicts of interest with the pharma industry that sells the vaccines or drugs that they are advertising. In Dr Higgins case although he doesn’t receive direct funding from pharma his whole (and short) publication history is dedicated to vaccine “nudging”, which the aforementioned hospital benefits a LOT from.
As a short aside it is worth noting this little doozy from Dave…

In total… 0.1% of neonates born at a planned home birth received HBV compared to 76.3% of neonates born in a hospital location… this translated to a large increase in the odds of not receiving HBV compared to in-hospital births (planned home birth (aOR: 502.05, 95% CI: 363.04-694.29).
Conclusions: Planned out-of-hospital birth is a risk factor for nonreceipt of the HBV birth dose. As births in these locations become more common, targeted policies and education are warranted
God forbid that women should dare to opt for a home birth to avoid the coercion our hospitals push to give your baby a Hepatitis B vaccine (that it doesn’t need unless it is going home to drug dealers or pedophiles).
And that is the person that wrote the article on measles. The public just gets to see this doctor-type authority and expect that they are telling the truth. But they are telling a distortion of the truth either because their funding stream relies on it, or they firmly believe the propaganda from generations of doctors funded by pharma.
Now back to the scariness (or not) of measles itself.
Firstly, measles is very far from “one of the deadliest infectious diseases” - that’s just a blatant lie. In developed countries the death rate is less than 1 per 1000 notified (i.e. symptomatic) cases. Many studies reported a zero case fatality rate, which is what it should be if children with measles were treated properly. I discussed this in my article about the manufactured epidemic of measles in Samoa in 2019, where the death rate was much higher than it should have been.

And secondly, the “measles is the most contagious disease on earth” claim is somewhat of a myth.
Let me show you why.
Measles for everyone
The idea sold to the public (as per the David Higgins example above) is that measles is the most contagious virus on earth.

“Contagious” usually denotes the ability to transmit a virus (or infection) to another person. Chicken pox is pretty contagious, meaning that most kids that come in contact with a chicken pox kid gets chicken pox. It’s a crude but effective form of vaccination - providing a contagious form of chicken pox from a healthy kid to another healthy kid.
But how contagious is measles really? Because we are told, repeatedly, that as the most contagious virus on earth its R0 is around 18.
The R0 value is the “basic reproduction number” and indicates the number of susceptible people that an infected person can infect.
The problem with an “R0 of 18” claim is that, very quickly, the whole population would be infected (and subsequently immune) if it was true - it’s not.
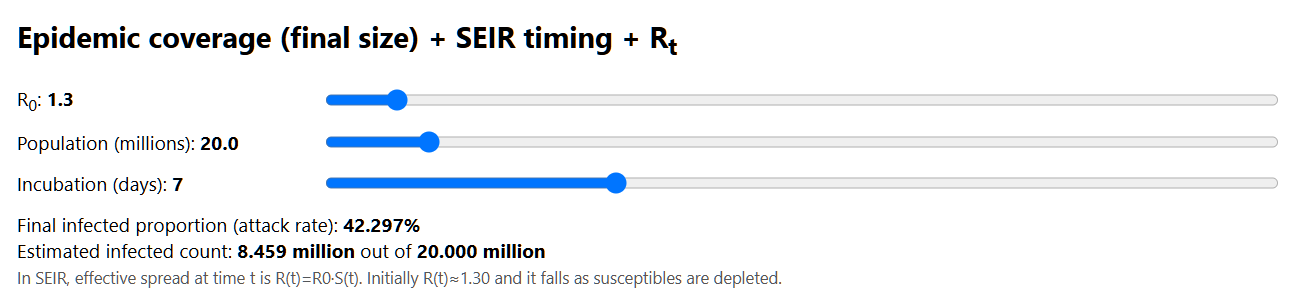
If you don’t believe me you can run this through this R0 calculator where you can set the population, incubation time and R0 and see how quickly it runs through the population.
For example, the Australian population around 2000 was about 20 million and if the R0 was truly 18 then 100% of the population would be infected in… about 2 months. Meaning, either the R0 isn’t anywhere near 18 or we never needed a vaccine (because everybody would be immune). Only one of those things can be true.

In fact, as you can see by playing with the calculator, any virus with an R0 of more than about 3.2 will provide herd immunity in any susceptible population.
So, can measles have an R0 of 18? Not a chance. Of course, this contention is based on modelling data (calculating what could happen in ideal circumstances), which a lot of “vaccine science” is based on. But what about what happens in the real world?
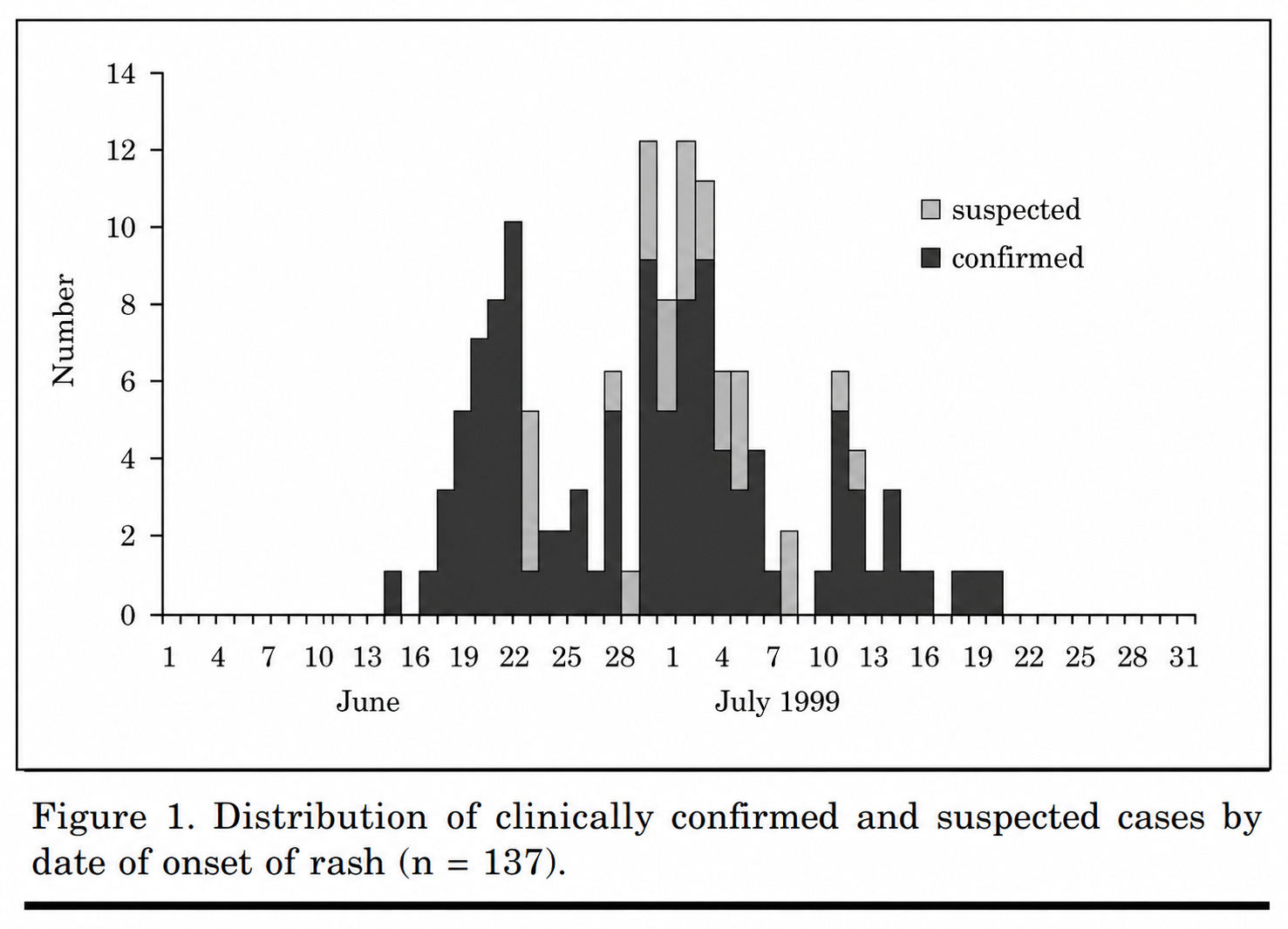
Well for that we really need a randomised or comparative trial - but, just like the measles vaccine itself, there isn’t one. The best we can do is the van den Hof study6 from the Netherlands published in 2001, which is actually quite informative. The study focused on an orthodox (Christian) school… presumably because “othering” the Jewish community was frowned upon at the time, the scientists moved their target for dirtyfication.
In this study the overall “attack rate” (which is the percentage of people that get the disease from someone else) was… 37%.
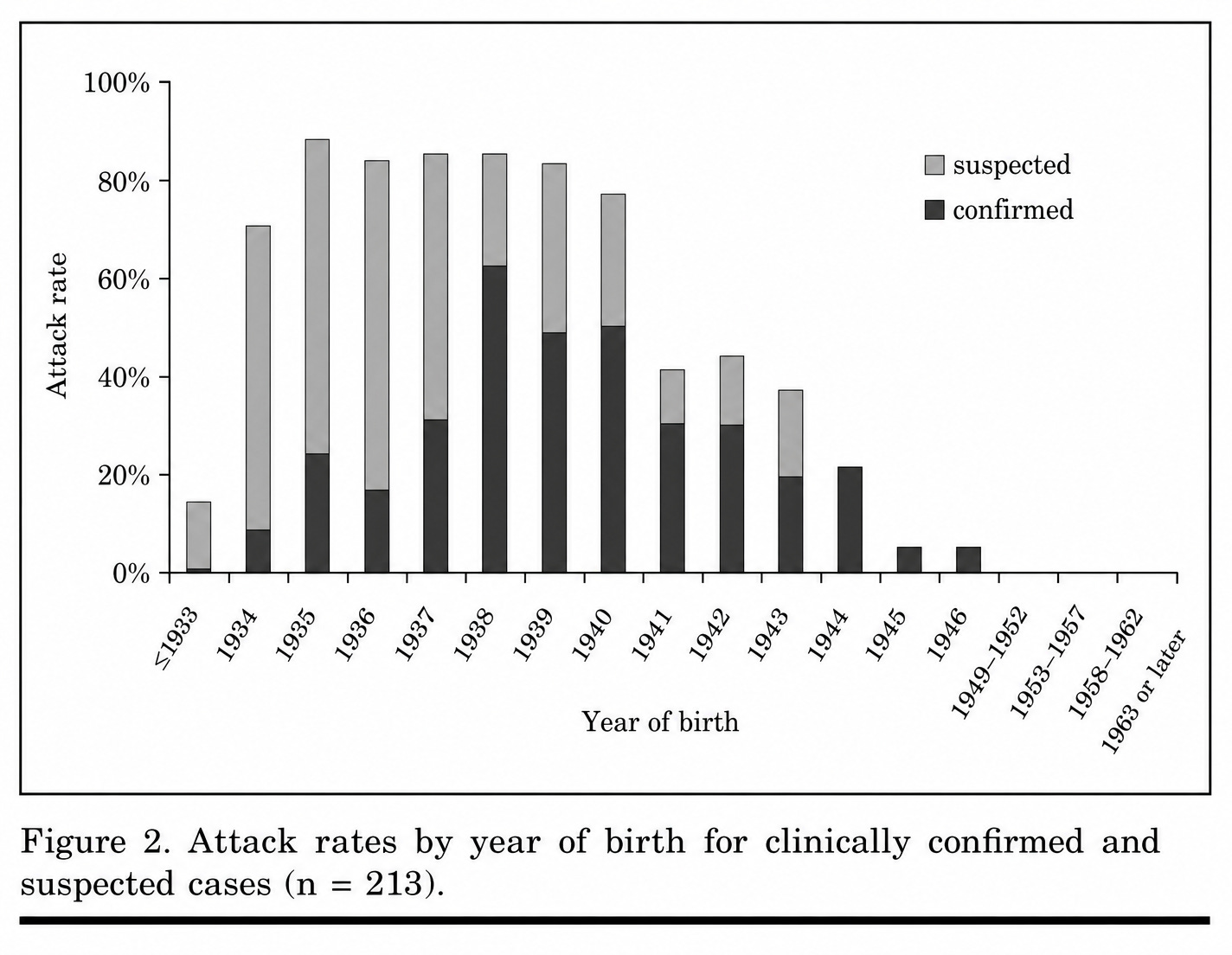
The authors make a note of the difference in attack rate by age to suggest that the younger non-immune are “at risk” of this dangerous disease. Like chickenpox then.
And what happened to these nearly 200 “unprotected” Christian kids?
Not much.
Of the 162 patients with confirmed or suspected measles who completed at least one questionnaire… one was hospitalized for delirium (Table 5).
Of the 22 children (who consulted a GP), 19 were given antibiotics: 9 for pneumonia, 9 for otitis media, and 1 for cystitis.
The complication rate did not differ between confirmed and suspected cases (26% vs. 24%).
The two things to note here are that there were no deaths - there was just one hospitalisation (0.6%) - and importantly those that got a chest infection (post-viral pneumonia) were correctly treated with antibiotics. Remember that this was banned during COVID, because, well, I guess some people needed to sell some things.
The same rule (treat post-viral pneumonia with appropriate antibiotics) applies to all types of post-viral pneumonia - highlighted in this awful case of medical negligence which was blamed on “measles”. The actual cause of death was a mycoplasma pneumonia that was incorrectly treated.

So, we have an unvaccinated cohort exposed to measles and a cumulative attack rate (transmission rate) of 37%. It should be realised that this cumulative attack rate (secondary, tertiary etc) doesn’t happen all at once. This is because there are reinfections in a localised population - of which the first infection (from which the R0 is calculated) is only about 40% of the total. This makes the actual secondary attack rate (transmission rate) in this study more like15%.
Irrespective, if we plug 37% into our calculator we actually get an R0 below 1.3, which is more likely to reflect the true transmission rate of measles - nothing at all like 18.
In fact, not only is there no real comparison study to establish the R0 of measles but there is also no randomised study showing that the measles infection conferred by vaccination is less likely to transmit to another person than natural infection.
So, again, we have no evidence that the measles vaccine (aka live measles infection) confers any less risk in any domain than a natural infection of measles.
And this is a good place to summarise where we are up to before the final leg of this little journey.
What have we discovered about the measles vaccine?
The measles vaccine is a live virus and gives children a viral illness
Making children take the measles vaccine (and therefore getting vaccine measles) doesn’t prevent measles any more than giving the children measles.
No controlled trial has established whether there was any benefit to injecting vaccine measles compared to injecting natural measles or being exposed to natural measles in the air.
The measles vaccine trials that we used in the 60s to establish the measles vaccine were conducted unethically in scenarios that contravened the Nuremberg code.
Measles is not “one of the most deadly and contagious infections known”. In fact only a minority of people exposed to measles will become infected with measles and if infected, nearly all people have a minor illness.
There is no controlled trial that shows that being infected naturally with measles is better or worse than being injected with vaccine measles.
This is a very different story from the one we normally get through the (pharma funded) media.
But there is another aspect established in the scientific realm that needs to be addressed, which is the impact of measles (vaccine) on mortality in the developing world.
Measles vaccine mortality reduction
One thing that could be difficult to explain without understanding that measles vaccine gives you measles is that there is reasonably good evidence that in developing countries, administration of the standard dose measles vaccine improves all-cause mortality.
Yes, you heard that right - although there is a caveat, a big one.
A number of studies performed by Peter Aaby and Christine Stabell-Benn over the last 30 years have shown that, in Africa at least, vaccination with measles vaccine is associated with a reduction in all-cause mortality.

That is, if a child is given a live measles virus by injection, that child has a lower risk of death in the subsequent few years than if the child doesn’t get a live measles virus by injection. Strange, right?
Even stranger when you consider the other vaccines - DTP mainly - are associated with the opposite effect, that is, a higher rate of all-cause mortality after vaccination. From the same research authors:

Note that, although the BMJ usually has its papers behind a paywall, the measles Aaby study (that shows a mortality benefit to the measles vaccine) is free to read, but the DTP Aaby study7 (the one that shows that the vaccine increases the risk of death) is behind a paywall in the journal vaccine. Just a coincidence, I’m sure.
For clarity, it is reasonably clear that, for whatever reason, giving a child a dose of measles improves their all-cause survival in developing countries. In fact, multiple studies (e.g. here and here) have shown that getting measles improves all-cause mortality.
For the record that’s measles, not measles vaccine.
And what that means is that it isn’t the measles vaccine providing this benefit, it’s the fact that you are giving the child measles when you inject them with… measles. And getting measles reduces your risk of dying of other diseases - at least in the developing world.
The reason for this is not known but it isn’t due to being protected against the not-very-lethal-at-all measles, as identified by the same authors:
Vaccine efficacy against death was much greater than the proportion of deaths attributed to acute measles disease. In four studies from Guinea-Bissau, Senegal, and Burundi vaccine efficacy against death remained almost unchanged when cases of measles were excluded from the analysis.
Diphtheria-tetanus-pertussis and polio vaccinations were not associated with reduction in mortality.
Interestingly this “beneficial” effect appears to be confined to live vaccines and, given that it it is also seen with “mild measles infection” one can reasonably assume that it is the fact that you are giving the child an infection that trains their immune system to fight other pathogens that provides the benefit.
In other words, measles infection has immune system benefits.
And, sure, you might be able to replicate these by giving a child measles by injection - but you’re just giving the kid measles, by injection.
“But It’s Attenuated Measles, not Measles”
Well, this is not only crux of this article but is central to the vaccine industry.
You see, the vaccine industry is claiming that their injected version of measles (and a number of other live virus vaccines) is “attenuated”. That means that it’s a “safe” version of measles.
But as we’ve seen… not only is real measles safe when managed correctly, providing an overall immunity boost benefit mostly for the price of a rash for a few days… the vaccine version of measles has the same effect. Because it’s live measles.
Essentially, they are claiming that their version of chicken-embryo-cell-derived measles is a safer version of measles and therefore you should inject their version into your child.
But is it any different from “real” measles?
No. And how do we know that?
We can look at their genome. In fact, Parks et al did this in 2001.

This paper is actually produced by the pharma company Wyeth, which was bought out by Pfizer - hence the Pearl River location. That’s the same Pearl River location that ran the COVID vaccine trial fraud that I wrote about extensively here:

They are of course proud of their products, and of how close they are to the original Edmonston measles strain - remember, the strain that did nothing to David Edmonston.

If you have time, you can use the lessons provided in the seminal article on BLAST that I published in 2021 to check out exactly how closely these strains are related. In other words, are they really different or are they do they just have the same level of difference that your flu virus strains have, but are still the same flu?
These are the BLAST results comparing all these vaccine (chicken) strains to the original measles. You can run it yourself by clicking here.
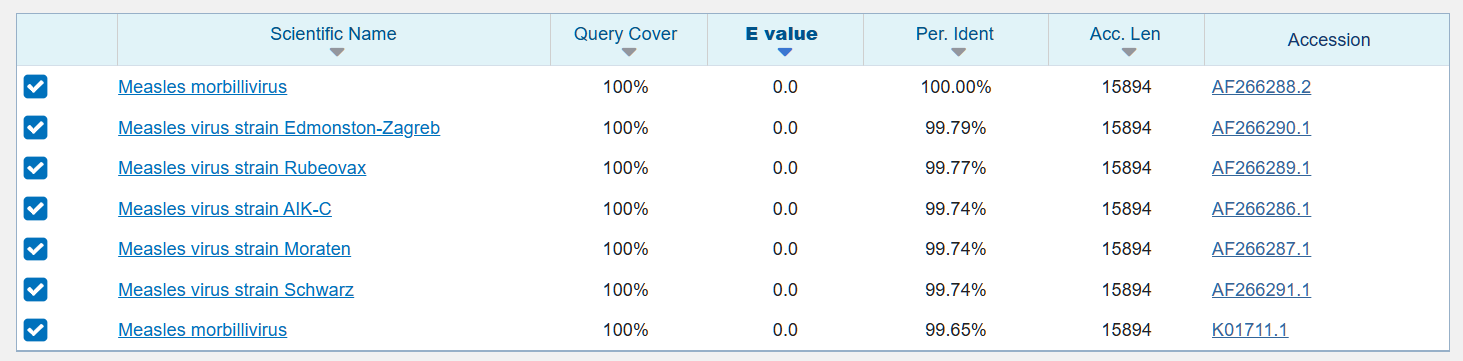
The “per ident” column provides the “percentage identity” and as you can see all these “vaccine” strains are less than 0.3% difference from the original measles. That’s essentially the same virus.
The sharp-eyed of you will have noticed that there are two entries for “measles morbillivirus” and that’s because the lower one, which is 99.65% identical to Edmonston, is just another strain of measles.
In other words, the genomic difference between the original measles and the vaccine versions of measles are less than the difference between strains of measles.
That’s because the vaccine strains are just measles. And they give your child measles. It’s just slightly different because it’s injected but it’s the same thing (and there is not a single controlled study to show otherwise).
Measles is measles. Chicken measles is also measles. Claiming it’s different just because it was grown in chicken eggs is a scam.
And just to drive home the point that chicken measles is measles.. Guess how different geographic versions of the exact same flu strain are from each other?
Here you are. This is a BLAST comparison of the HA antigens from differently annotations of the exact same flu virus - pandemic 2009 H1N1. For those not paying attention over the last 6 years that’s the one they have been putting in flu vaccines since, well, 2009 (when it was presumably created to sell the pandemrix vaccine).
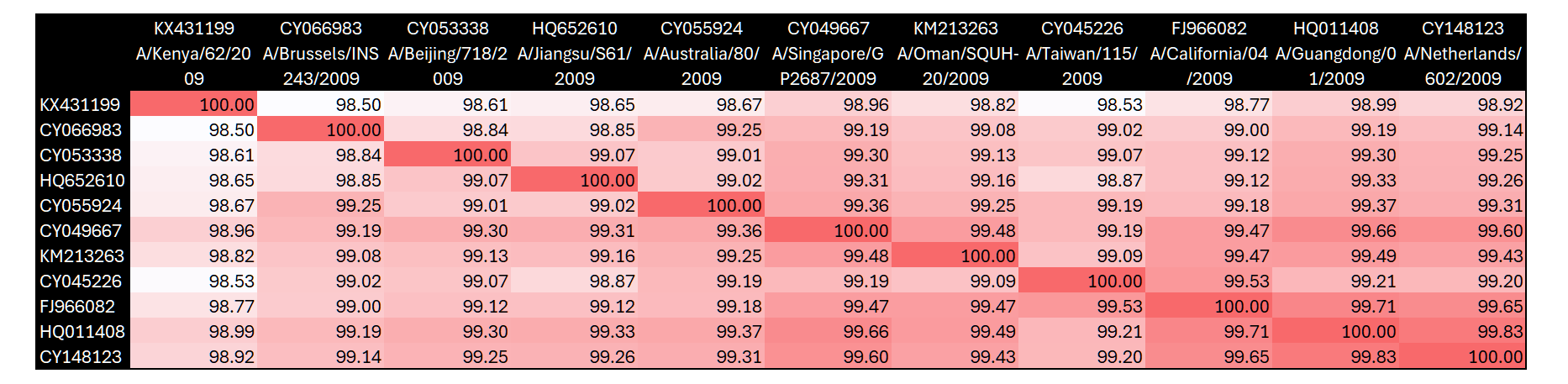
The heat map shows that these exact same viruses (including the vaccine version) have a similarity of 98.5% to 99.83%, or a difference of 0.17% to 1.5%.
In other words there is far more similarity between vaccine strains of measles then there is between the exact same year’s strain of the flu.
In other words, the measles vaccine, chicken measles, human measles… are all the same.
And the only difference is that they were injected into kids (bypassing a lot of the immune response) instead of inhaled or ingested, so they produce a slightly different symptom set.
The vaccine industry has been selling you “attenuated” vaccines for over 60 years, and everybody fell for it.
But they just gave you measles in a syringe.
And made a fortune.
For those interested in the political history of vaccine propaganda and coercion, the wayout substack’s excellent article is a riveting read.
Enders et al, Studies on an Attenuated Measles-Virus Vaccine, NEJM 1960
Morley et al Journal of Hygiene 1963.
Very, very, very well said!
Wow, what an outstanding post. Topnotch.